

Sulopenem or Ciprofloxacin for the Treatment of Uncomplicated Urinary Tract Infections in Women: A Phase 3, Randomized Trial
- PMID: 36069202
- PMCID: PMC9825825
- DOI: 10.1093/cid/ciac738
Sulopenem or Ciprofloxacin for the Treatment of Uncomplicated Urinary Tract Infections in Women: A Phase 3, Randomized Trial
Erratum in
-
Correction to: Sulopenem or Ciprofloxacin for the Treatment of Uncomplicated Urinary Tract Infections in Women: A Phase 3, Randomized Trial.Clin Infect Dis. 2023 Sep 18;77(6):937. doi: 10.1093/cid/ciad216. Clin Infect Dis. 2023. PMID: 37590314 Free PMC article. No abstract available.
Abstract
Background: There are limited treatment options for uncomplicated urinary tract infection (uUTI) caused by resistant pathogens. Sulopenem etzadroxil/probenecid (sulopenem) is an oral thiopenem antibiotic active against multidrug-resistant pathogens that cause uUTIs.
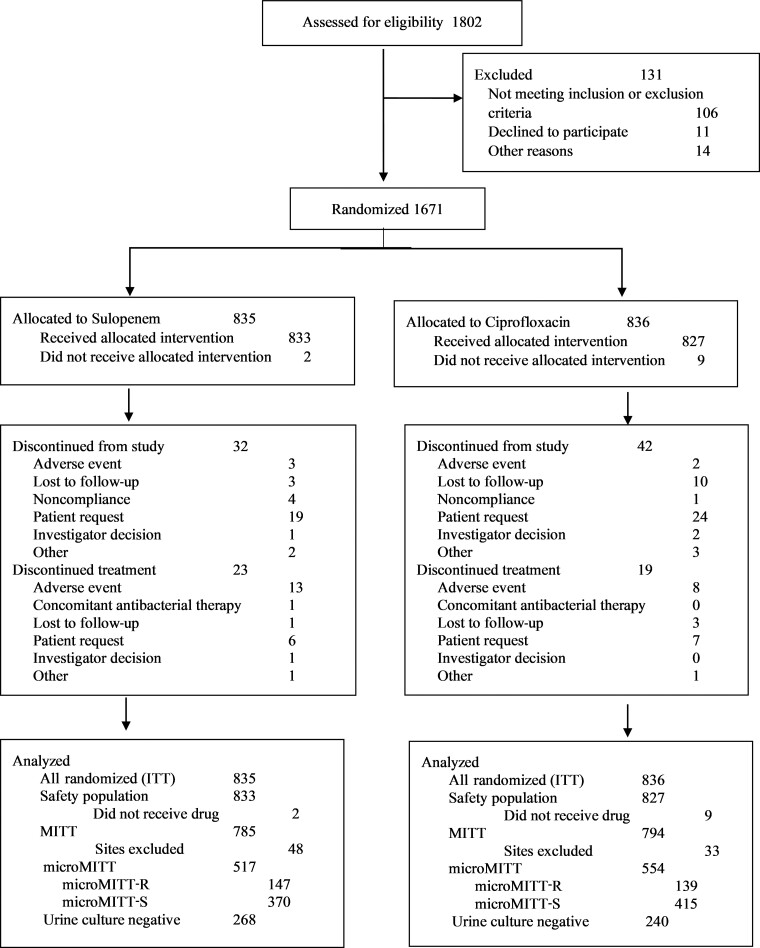
Methods: Patients with uUTI were randomized to 5 days of sulopenem or 3 days of ciprofloxacin. The primary endpoint was overall success, defined as both clinical and microbiologic response at day 12. In patients with ciprofloxacin-nonsusceptible baseline pathogens, sulopenem was compared for superiority over ciprofloxacin; in patients with ciprofloxacin-susceptible pathogens, the agents were compared for noninferiority. Using prespecified hierarchical statistical testing, the primary endpoint was tested in the combined population if either superiority or noninferiority was declared in the nonsusceptible or susceptible population, respectively.
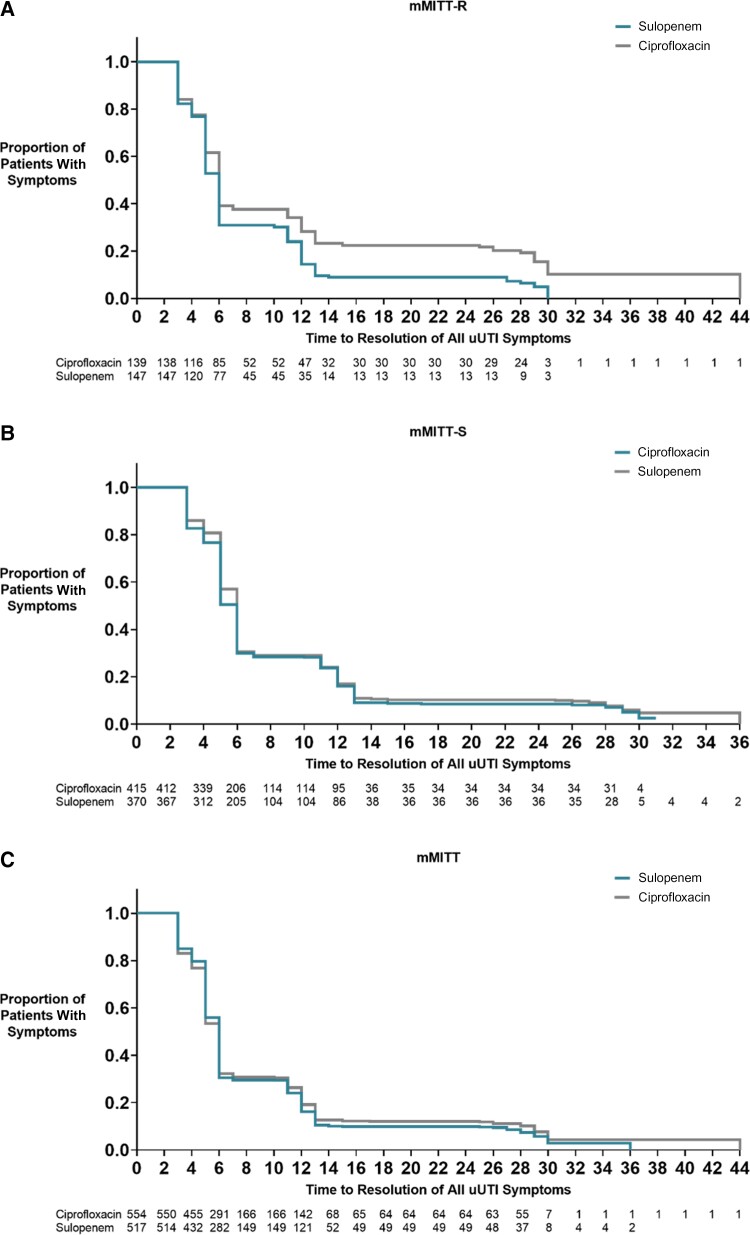
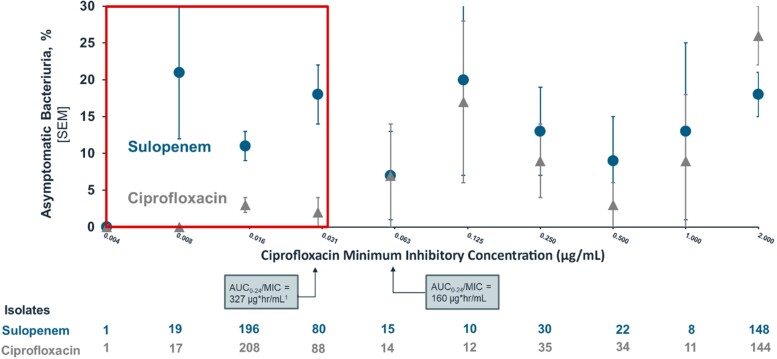
Results: In the nonsusceptible population, sulopenem was superior to ciprofloxacin, 62.6% vs 36.0% (difference, 26.6%; 95% confidence interval [CI], 15.1 to 7.4; P <.001). In the susceptible population, sulopenem was not noninferior to ciprofloxacin, 66.8% vs 78.6% (difference, -11.8%; 95% CI, -18.0 to 5.6). The difference was driven by a higher rate of asymptomatic bacteriuria (ASB) post-treatment in patients on sulopenem. In the combined analysis, sulopenem was noninferior to ciprofloxacin, 65.6% vs 67.9% (difference, -2.3%; 95% CI, -7.9 to 3.3). Diarrhea occurred more frequently with sulopenem (12.4% vs 2.5%).
Conclusions: Sulopenem was noninferior to ciprofloxacin in the treatment of uUTIs. Sulopenem was superior to ciprofloxacin in patients with uUTIs due to ciprofloxacin-nonsusceptible pathogens. Sulopenem was not noninferior in patients with ciprofloxacin-susceptible pathogens, driven largely by a lower rate of ASB in those who received ciprofloxacin.
Clinical trial registration: NCT03354598.
Keywords: sulopenem; uncomplicated urinary tract infection.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. M. W. D., S. I. A., S. P., K. A., and M. T. Z. report being employees of Iterum Therapeutics during the conduct of the study and owning stock in Iterum Therapeutics. A. F. D. reports receiving consulting fees from Iterum Therapeutics, ContraFect, UTILITY, MicuRX, and Paratek, including serving on a data and safety monitoring board for Paratek. H. W. B. reports consulting fees and serving as associate editor of Antimicrobial Agents and Chemotherapy and editor of Infectious Diseases Clinics of North America and Sanford Guide. M. W. D. reports patents pending from Iterum Therapeutics and serving on the Iterum Therapeutics Board of Directors. S. P. reports consulting fees and being an employee and stockholder of Iterum Therapeutics, the sponsor for this study. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011; 52:e103–20. - PubMed
-
- Fihn SD. Acute uncomplicated urinary tract infection in women. N Engl J Med 2003; 349:259–66. - PubMed
-
- Talan DA, Takhar SS, Krishnadasan A, et al. Emergence of extended-spectrum β-lactamase urinary tract infections among hospitalized emergency department patients in the United States. Ann Emerg Med 2021; 77:32–43. - PubMed
