

Effective Rapid Diagnosis of Bacterial and Fungal Bloodstream Infections by T2 Magnetic Resonance Technology in the Pediatric Population
- PMID: 36069557
- PMCID: PMC9580347
- DOI: 10.1128/jcm.00292-22
Effective Rapid Diagnosis of Bacterial and Fungal Bloodstream Infections by T2 Magnetic Resonance Technology in the Pediatric Population
Abstract
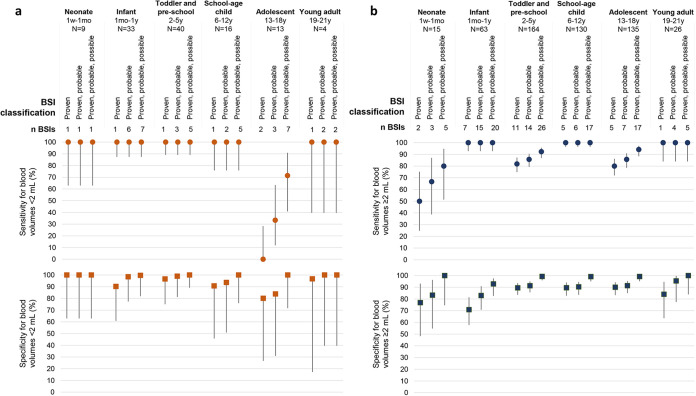
Children are prone to bloodstream infections (BSIs), the rapid and accurate diagnosis of which is an unmet clinical need. The T2MR technology is a direct molecular assay for identification of BSI pathogens, which can help to overcome the limits of blood culture (BC) such as diagnostic accuracy, blood volumes required, and turnaround time. We analyzed results obtained with the T2Bacteria (648) and T2Candida (106) panels in pediatric patients of the Bambino Gesù Children's Hospital between May 2018 and September 2020 in order to evaluate the performance of the T2Dx instrument with respect to BC. T2Bacteria and T2Candida panels showed 84.2% and 100% sensitivity with 85.9% and 94.1% specificity, respectively. The sensitivity and specificity of the T2Bacteria panel increased to 94.9% and 98.7%, respectively, when BC was negative but other laboratory data supported the molecular result. T2Bacteria sensitivity was 100% with blood volumes <2 mL in neonates and infants. T2Bacteria and T2Candida provided definitive microorganism identification in a mean time of 4.4 and 3.7 h, respectively, versus 65.7 and 125.5 h for BCs (P < 0.001). T2 panels rapidly and accurately enable a diagnosis of a pediatric BSI, even in children under 1 year of age and for very small blood volumes. These findings support their clinical use in life-threatening pediatric infections, where the time to diagnosis is of utmost importance, in order to improve survival and minimize the long-term sequalae of sepsis. The T2 technology could be further developed to include more bacteria and fungi species that are involved in the etiology of sepsis.
Keywords: T2 magnetic resonance; T2 panels; bloodstream infections; molecular diagnosis; pediatric population.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, Colombara DV, Ikuta KS, Kissoon N, Finfer S, Fleischmann-Struzek C, Machado FR, Reinhart KK, Rowan K, Seymour CW, Watson RS, West TE, Marinho F, Hay SI, Lozano R, Lopez AD, Angus DC, Murray CJL, Naghavi M. 2020. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet Lond Engl 395:200–211. 10.1016/S0140-6736(19)32989-7. - DOI - PMC - PubMed
-
- Köstlin-Gille N, Härtel C, Haug C, Göpel W, Zemlin M, Müller A, Poets CF, Herting E, Gille C. 2021. Epidemiology of early and late onset neonatal sepsis in very low birthweight infants: data from the German Neonatal Network. Pediatr Infect Dis J 40:255–259. 10.1097/INF.0000000000002976. - DOI - PubMed
-
- Zingg W, Hopkins S, Gayet-Ageron A, Holmes A, Sharland M, Suetens C, ECDC PPS study group . 2017. Health-care-associated infections in neonates, children, and adolescents: an analysis of paediatric data from the European Centre for Disease Prevention and Control point-prevalence survey. Lancet Infect Dis 17:381–389. 10.1016/S1473-3099(16)30517-5. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
