

Exploring the Cystic Fibrosis Lung Microbiome: Making the Most of a Sticky Situation
- PMID: 36069903
- PMCID: PMC9451016
- DOI: 10.1093/jpids/piac036
Exploring the Cystic Fibrosis Lung Microbiome: Making the Most of a Sticky Situation
Abstract
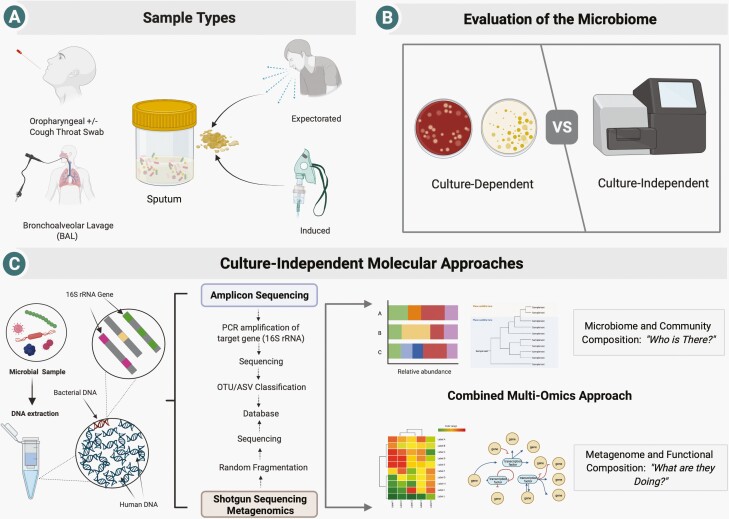
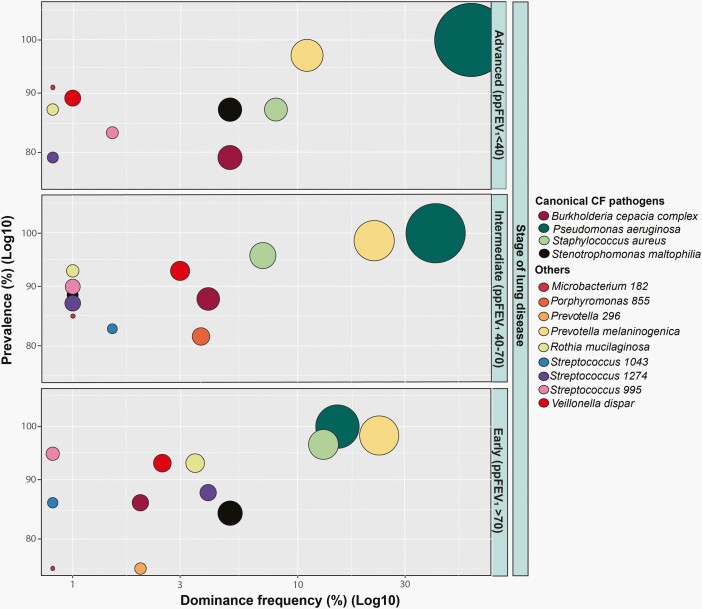
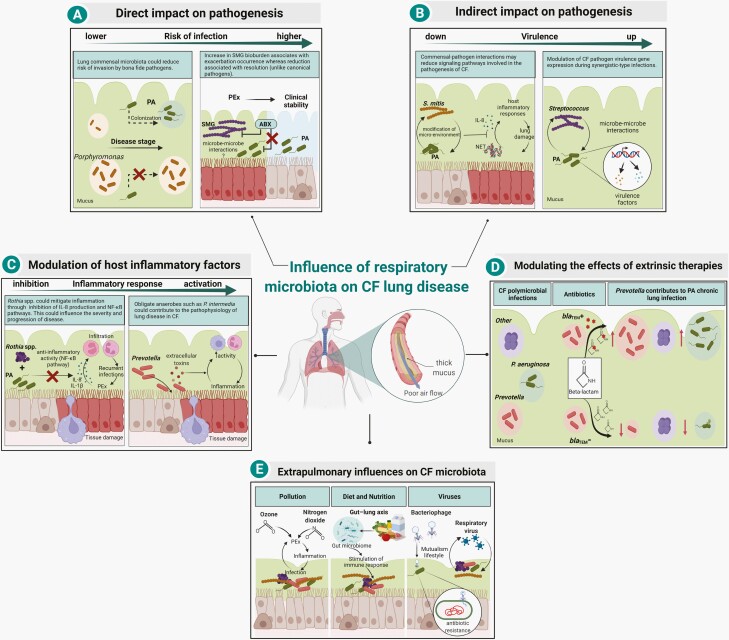
Chronic lower respiratory tract infections are a leading contributor to morbidity and mortality in persons with cystic fibrosis (pwCF). Traditional respiratory tract surveillance culturing has focused on a limited range of classic pathogens; however, comprehensive culture and culture-independent molecular approaches have demonstrated complex communities highly unique to each individual. Microbial community structure evolves through the lifetime of pwCF and is associated with baseline disease state and rates of disease progression including occurrence of pulmonary exacerbations. While molecular analysis of the airway microbiome has provided insight into these dynamics, challenges remain including discerning not only "who is there" but "what they are doing" in relation to disease progression. Moreover, the microbiome can be leveraged as a multi-modal biomarker for both disease activity and prognostication. In this article, we review our evolving understanding of the role these communities play in pwCF and identify challenges in translating microbiome data to clinical practice.
Keywords: Pseudomonas aeruginosa; biomarker; bronchiectasis; lung; microbiota; review.
© The Author(s) 2022. Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society.
Figures
Similar articles
-
Microbial Epidemiology of the Cystic Fibrosis Airways: Past, Present, and Future.Semin Respir Crit Care Med. 2023 Apr;44(2):269-286. doi: 10.1055/s-0042-1758732. Epub 2023 Jan 9. Semin Respir Crit Care Med. 2023. PMID: 36623820 Review.
-
Supplemental Oxygen Alters the Airway Microbiome in Cystic Fibrosis.mSystems. 2022 Oct 26;7(5):e0036422. doi: 10.1128/msystems.00364-22. Epub 2022 Aug 24. mSystems. 2022. PMID: 36000724 Free PMC article.
-
The cystic fibrosis lung microbiome.Ann Am Thorac Soc. 2014 Jan;11 Suppl 1:S61-5. doi: 10.1513/AnnalsATS.201306-159MG. Ann Am Thorac Soc. 2014. PMID: 24437409
-
Sputum microbiota is predictive of long-term clinical outcomes in young adults with cystic fibrosis.Thorax. 2018 Nov;73(11):1016-1025. doi: 10.1136/thoraxjnl-2018-211510. Epub 2018 Aug 22. Thorax. 2018. PMID: 30135091
-
The microbiome and emerging pathogens in cystic fibrosis and non-cystic fibrosis bronchiectasis.Semin Respir Crit Care Med. 2015 Apr;36(2):225-35. doi: 10.1055/s-0035-1546752. Epub 2015 Mar 31. Semin Respir Crit Care Med. 2015. PMID: 25826590 Review.
Cited by
-
The Impact of Antimicrobial Resistance in Cystic Fibrosis.J Clin Med. 2024 Mar 16;13(6):1711. doi: 10.3390/jcm13061711. J Clin Med. 2024. PMID: 38541936 Free PMC article. Review.
-
Insights into the role of the respiratory tract microbiome in defense against bacterial pneumonia.Curr Opin Microbiol. 2024 Feb;77:102428. doi: 10.1016/j.mib.2024.102428. Epub 2024 Jan 25. Curr Opin Microbiol. 2024. PMID: 38277901 Free PMC article. Review.
-
Exploring the role of microbiome in cystic fibrosis clinical outcomes through a mediation analysis.mSystems. 2025 Jun 17;10(6):e0019625. doi: 10.1128/msystems.00196-25. Epub 2025 May 28. mSystems. 2025. PMID: 40434093 Free PMC article.
-
Highly Effective Modulator Therapy: Implications for the Microbial Landscape in Cystic Fibrosis.Int J Mol Sci. 2024 Nov 5;25(22):11865. doi: 10.3390/ijms252211865. Int J Mol Sci. 2024. PMID: 39595943 Free PMC article. Review.
-
Antibacterial and Antibiofilm Effects of Lactobacilli Strains against Clinical Isolates of Pseudomonas aeruginosa under Conditions Relevant to Cystic Fibrosis.Antibiotics (Basel). 2023 Jul 7;12(7):1158. doi: 10.3390/antibiotics12071158. Antibiotics (Basel). 2023. PMID: 37508254 Free PMC article.
References
-
- Rogers GB, Hart CA, Mason JR, Hughes M, Walshaw MJ, Bruce KD.. Bacterial diversity in cases of lung infection in cystic fibrosis patients: 16S ribosomal DNA (rDNA) length heterogeneity PCR and 16S rDNA terminal restriction fragment length polymorphism profiling. J Clin Microbiol 2003; 41:3548–58. - PMC - PubMed
-
- Duan K, Dammel C, Stein J, Rabin H, Surette MG.. Modulation of Pseudomonas aeruginosa gene expression by host microflora through interspecies communication. Mol Microbiol 2003; 50:1477–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
