

International pooled patient-level meta-analysis of ketamine infusion for depression: In search of clinical moderators
- PMID: 36071111
- PMCID: PMC9763119
- DOI: 10.1038/s41380-022-01757-7
International pooled patient-level meta-analysis of ketamine infusion for depression: In search of clinical moderators
Abstract
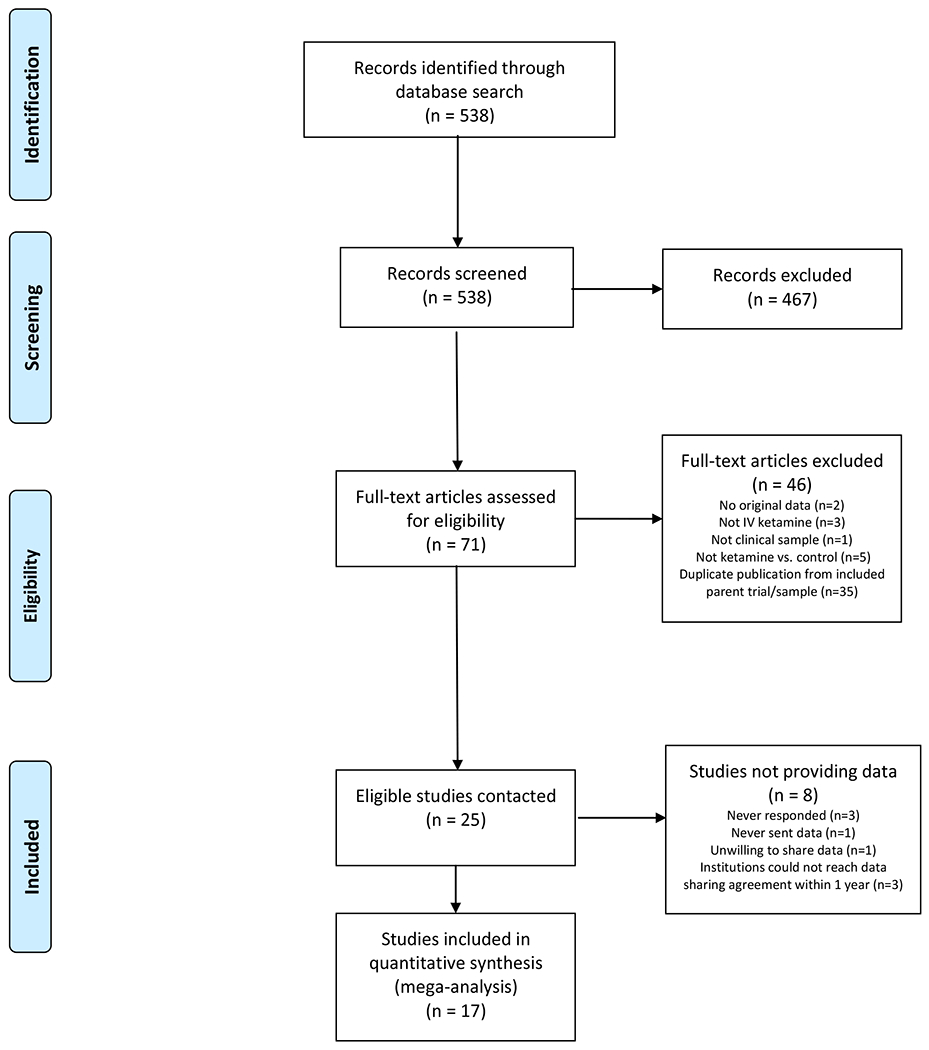
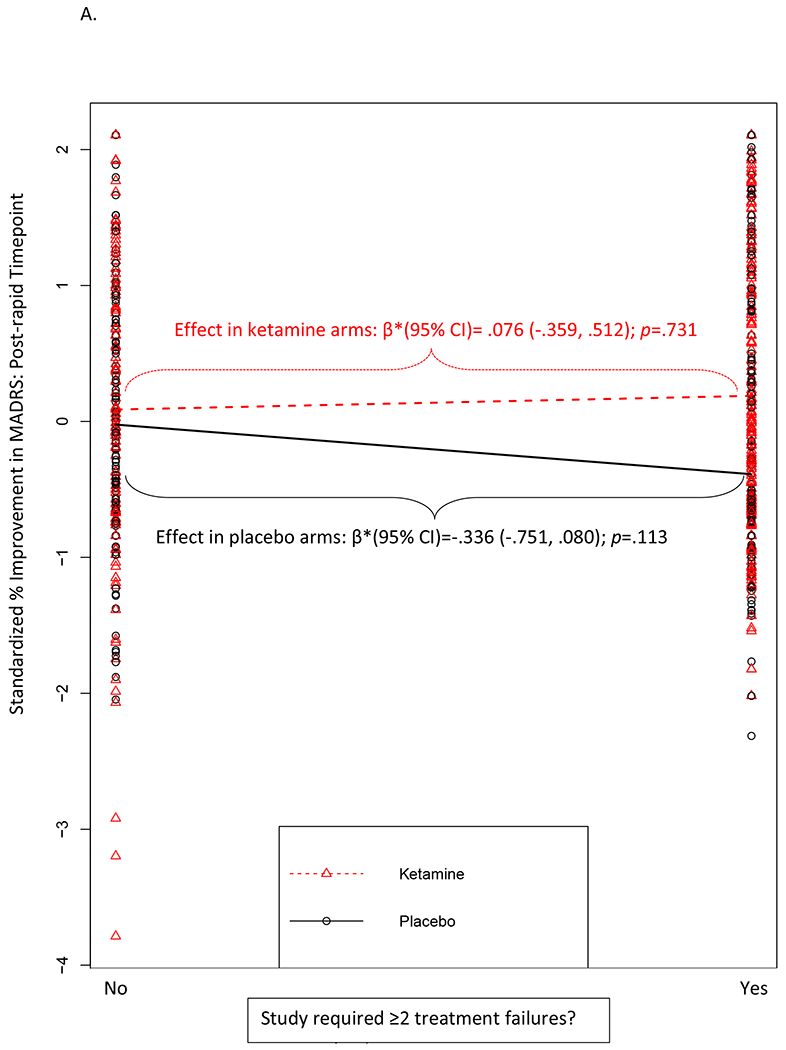
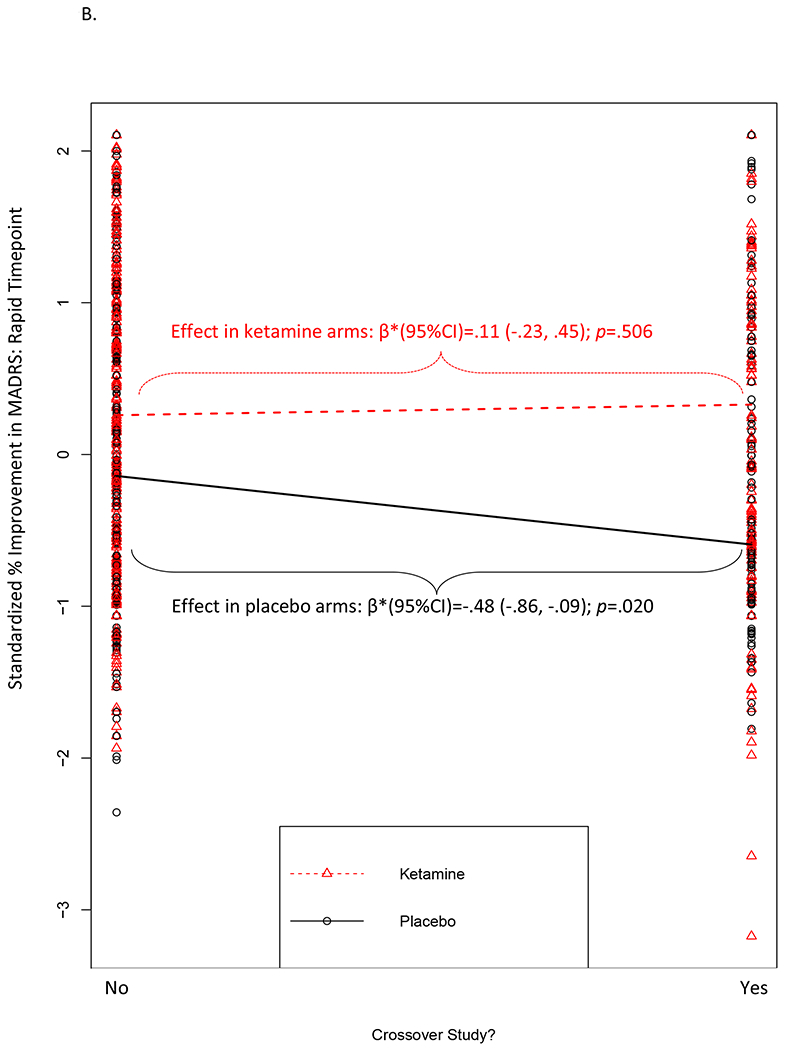
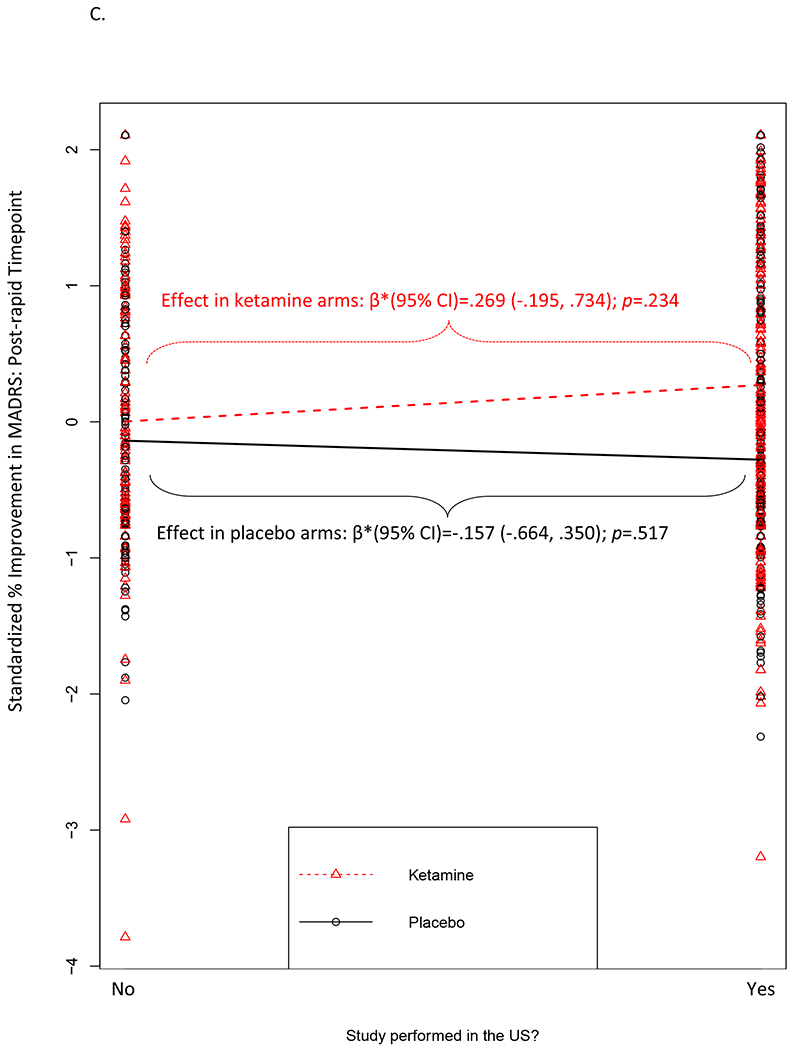
Depression is disabling and highly prevalent. Intravenous (IV) ketamine displays rapid-onset antidepressant properties, but little is known regarding which patients are most likely to benefit, limiting personalized prescriptions. We identified randomized controlled trials of IV ketamine that recruited individuals with a relevant psychiatric diagnosis (e.g., unipolar or bipolar depression; post-traumatic stress disorder), included one or more control arms, did not provide any other study-administered treatment in conjunction with ketamine (although clinically prescribed concurrent treatments were allowable), and assessed outcome using either the Montgomery-Åsberg Depression Rating Scale or the Hamilton Rating Scale for Depression (HRSD-17). Individual patient-level data for at least one outcome was obtained from 17 of 25 eligible trials [pooled n = 809]. Rates of participant-level data availability across 33 moderators that were solicited from these 17 studies ranged from 10.8% to 100% (median = 55.6%). After data harmonization, moderators available in at least 40% of the dataset were tested sequentially, as well as with a data-driven, combined moderator approach. Robust main effects of ketamine on acute [~24-hours; β*(95% CI) = 0.58 (0.44, 0.72); p < 0.0001] and post-acute [~7 days; β*(95% CI) = 0.38 (0.23, 0.54); p < 0.0001] depression severity were observed. Two study-level moderators emerged as significant: ketamine effects (relative to placebo) were larger in studies that required a higher degree of previous treatment resistance to federal regulatory agency-approved antidepressant medications (≥2 failed trials) for study entry; and in studies that used a crossover design. A comprehensive data-driven search for combined moderators identified statistically significant, but modest and clinically uninformative, effects (effect size r ≤ 0.29, a small-medium effect). Ketamine robustly reduces depressive symptoms in a heterogeneous range of patients, with benefit relative to placebo even greater in patients more resistant to prior medications. In this largest effort to date to apply precision medicine approaches to ketamine treatment, no clinical or demographic patient-level features were detected that could be used to guide ketamine treatment decisions.Review Registration: PROSPERO Identifier: CRD42021235630.
© 2022. The Author(s).
Figures
References
-
- Caddy C, Amit BH, McCloud TL, Rendell JM, Furukawa TA, McShane R, et al. Ketamine and other glutamate receptor modulators for depression in adults. Cochrane Database Syst Rev. 2015;Sep 23(9):CD011612. - PubMed
-
- McCloud TL, Caddy C, Jochim J, Rendell JM, Diamond PR, Shuttleworth C, et al. Ketamine and other glutamate receptor modulators for depression in bipolar disorder in adults. Cochrane Database Syst Rev. 2015(9):CD011611. - PubMed
-
- Schatzberg AF: A word to the wise about ketamine. Am J Psychiatry. 2014;171(3):262–4. - PubMed
