

Looking for the best strategy to treat children with new onset juvenile idiopathic arthritis: presentation of the "comparison of STep-up and step-down therapeutic strategies in childhood ARthritiS" (STARS) trial
- PMID: 36071444
- PMCID: PMC9450438
- DOI: 10.1186/s12969-022-00739-x
Looking for the best strategy to treat children with new onset juvenile idiopathic arthritis: presentation of the "comparison of STep-up and step-down therapeutic strategies in childhood ARthritiS" (STARS) trial
Abstract
Background: Although a satisfactory disease control is nowadays achievable in most patients with JIA, a substantial proportion of them still do not respond adequately or reach long-term drug-free remission. According to current recommendations, treatment should be escalated in subsequent steps. A different approach is based on the assumption that the initial start of an aggressive therapy may take advantage of the "window of opportunity" and could alter the biology of the disease, leading to an improvement of long-term outcomes, including the prevention of cumulative joint damage.
Objectives: This randomised clinical trial aims to compare the effectiveness of a conventional therapeutic regimen, based on treatment escalation and driven by the treat-to-target approach, with that of an early aggressive intervention based on the initial start of a combination of conventional and biological DMARDs.
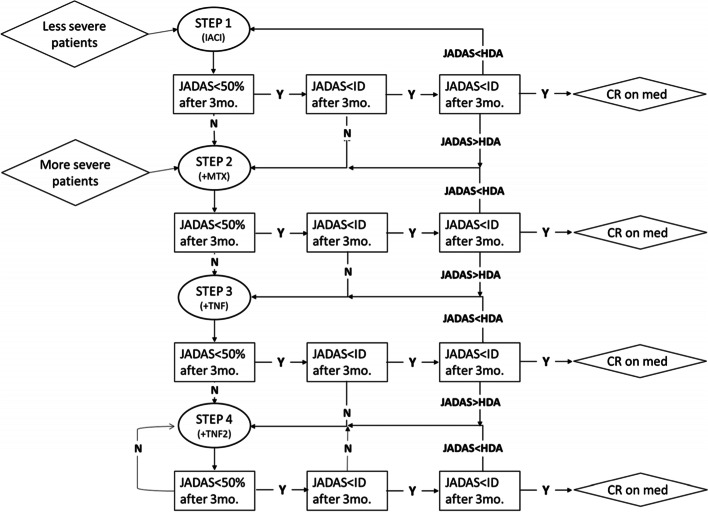
Methods: JIA patients with oligoarthritis or RF negative polyarthritis aged more than 2 years and with less than 4 months of disease course will be included in the study. Children will be randomised into two arms: patients in Step-up arm with less severe oligoarthritis will undergo an intra-articular corticosteroid injection (IACI) in all affected joints; patients with polyarthritis or severe oligoarthritis will receive IACI and methotrexate. Subsequent treatment will follow a standardised protocol based on the patients' level of disease activity measured with the JADAS, according to a treat-to-target strategy. Patients in Step-down arm will receive a 6-month early combined treatment (methotrexate plus IACI for less severe oligoarthritis, methotrexate plus etanercept for severe oligoarthritis and polyarthritis). The primary endpoint is the frequency of achievement of the status of clinical remission (i.e. persistence of inactive disease for at least 6 months) at the 12-month visit. Safety events, physician-centred measures and parent/patient-reported outcomes will be collected through the Paediatric Rheumatology International Trials Organisation on line database.
Expected results: The STARS trial aims to provide important evidence supporting the first-line treatment choices in the care of children with oligoarticular and polyarticular JIA. If the superiority of an early aggressive therapy will be demonstrated, this will demand further studies on the biological definition of the window of opportunity for JIA.
Trial registration: The Trial is registered on the ClinicalTrials.gov registry (NCT03728478) on the 31st October 2018 and EU Clinical Trials Register on the 14th May 2018 (EudraCT Number: 2018-001931-27).
Keywords: Anti-TNF; Juvenile idiopathic arthritis; Methotrexate; Randomised clinical trial; Treat-to target.
© 2022. The Author(s).
Conflict of interest statement
Marco Burrone, Marta Mazzoni, Roberta Naddei, Angela Pistorio, Maddalena Spelta, Marco Garrone, Maria Lombardi, Elisa Patrone, Silvia Scala, Luca Villa have no conflicts of interest to disclose.
Nicolino Ruperto has received honoraria for consultancies or speaker bureaus from the following pharmaceutical companies in the past 3 years: 2 Bridge, Amgen, AstraZeneca, Aurinia, Bayer, Brystol Myers and Squibb, Celgene, inMed, Cambridge Healthcare Research, Domain Therapeutic, EMD Serono, Glaxo Smith Kline, Idorsia, Janssen, Eli Lilly, Novartis, Pfizer, Sobi, UCB.
The IRCCS Istituto Giannina Gaslini (IGG), where NR works as full-time public employee, has received contributions from the following industries in the last 3 years: Bristol Myers and Squibb, Eli-Lilly, F Hoffmann-La Roche, Novartis, Pfizer, Sobi. This funding has been reinvested for the research activities of the hospital in a fully independent manner, without any commitment with third parties.
Angelo Ravelli has received honoraria for consultancies or speaker bureaus from the following pharmaceutical companies in the past 3 years: AbbVie, Angelini, BMS, Pfizer, Hoffman LaRoche, Novartis, Pfizer, Reckitt Benckiser.
Alessandro Consolaro reports Investigator initiated research grant from Pfizer and Alfa Sigma and speaker’s bureaus from Pfizer.
Figures

References
-
- Beukelman T, Patkar NM, Saag KG, Tolleson-Rinehart S, Cron RQ, DeWitt EM, et al. 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and safety monitoring of therapeutic agents for the treatment of arthritis and systemic features. Arthritis Care Res. 2011;63(4):465–482. doi: 10.1002/acr.20460. - DOI - PMC - PubMed
-
- Smolen JS. Treat-to-target: rationale and strategies. Clin Exp Rheumatol. 2012;30(4 Suppl 73):S2–S6. - PubMed
-
- Ravelli A, Consolaro A, Horneff G, Laxer RM, Lovell DJ, Wulffraat NM, et al. Treating juvenile idiopathic arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2018;77(6):819–828. - PubMed
-
- Smolen JS, Landewé R, Breedveld FC, Dougados M, Emery P, Gaujoux-Viala C, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann Rheum Dis. 2010;69(6):964–975. doi: 10.1136/ard.2009.126532. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
