

In vivo assessment of Lewy body and beta-amyloid copathologies in idiopathic normal pressure hydrocephalus: prevalence and associations with clinical features and surgery outcome
- PMID: 36071460
- PMCID: PMC9454182
- DOI: 10.1186/s12987-022-00368-2
In vivo assessment of Lewy body and beta-amyloid copathologies in idiopathic normal pressure hydrocephalus: prevalence and associations with clinical features and surgery outcome
Abstract
Background: Idiopathic normal pressure hydrocephalus (iNPH) is a clinico-radiological syndrome of elderly individuals likely sustained by different neurodegenerative changes as copathologies. Since iNPH is a potentially reversible condition, assessing neurodegenerative pathologies in vitam through CSF biomarkers and their influence on clinical features and surgical outcome represents crucial steps.
Methods: We measured α-synuclein seeding activity related to Lewy body (LB) pathology by the real-time quaking-induced conversion assay (RT-QuIC) and Alzheimer disease core biomarkers (proteins total-tau, phospho-tau, and amyloid-beta) by immunoassays in the cerebrospinal fluid (CSF) of 293 iNPH patients from two independent cohorts. To compare the prevalence of LB copathology between iNPH participants and a control group representative of the general population, we searched for α-synuclein seeding activity in 89 age-matched individuals who died of Creutzfeldt-Jakob disease (CJD). Finally, in one of the iNPH cohorts, we also measured the CSF levels of neurofilament light chain protein (NfL) and evaluated the association between all CSF biomarkers, baseline clinical features, and surgery outcome at 6 months.
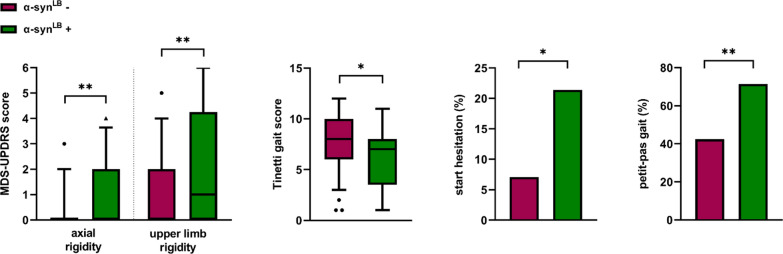
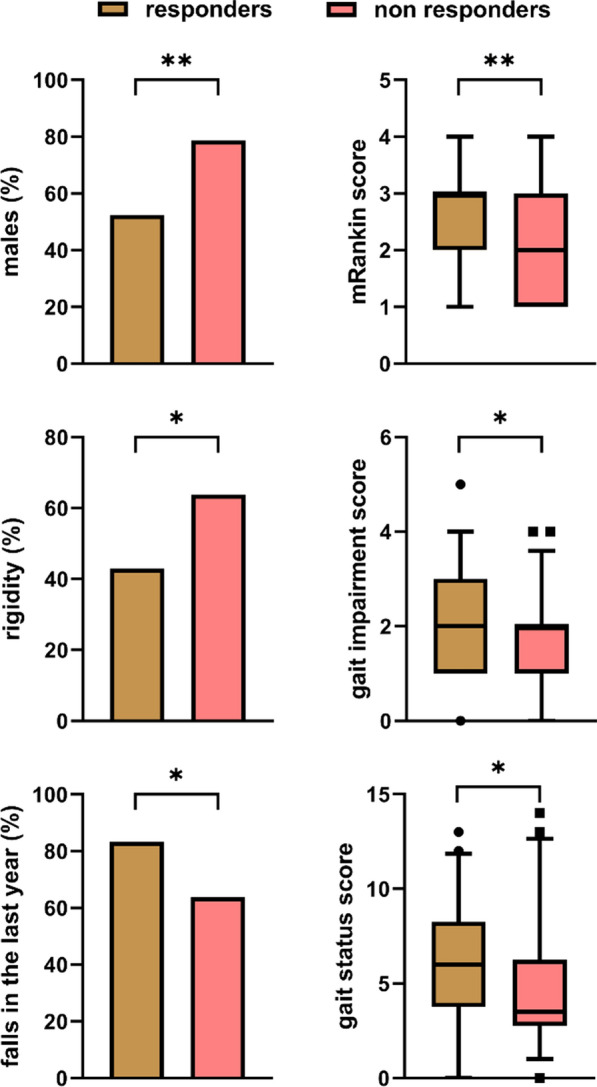
Results: Sixty (20.5%) iNPH patients showed α-synuclein seeding activity with no significant difference between cohorts. In contrast, the prevalence observed in CJD was only 6.7% (p = 0.002). Overall, 24.0% of iNPH participants showed an amyloid-positive (A+) status, indicating a brain co-pathology related to Aβ deposition. At baseline, in the Italian cohort, α-synuclein RT-QuIC positivity was associated with higher scores on axial and upper limb rigidity (p = 0.003 and p = 0.011, respectively) and lower MMSEc scores (p = 0.003). A+ patients showed lower scores on the MMSEc (p = 0.037) than A- patients. Higher NfL levels were also associated with lower scores on the MMSEc (rho = -0.213; p = 0.021). There were no significant associations between CSF biomarkers and surgical outcome at 6 months (i.e. responders defined by decrease of 1 point on the mRankin scale).
Conclusions: Prevalent LB- and AD-related neurodegenerative pathologies affect a significant proportion of iNPH patients and contribute to cognitive decline (both) and motor impairment (only LB pathology) but do not significantly influence the surgical outcome at 6 months. Their effect on the clinical benefit after surgery over a more extended period remains to be determined.
Keywords: Biomarkers; Cerebrospinal fluid; Idiopathic normal pressure hydrocephalus; Lewy body; Movement disorders; RT-QuIC; Real-time quaking-induced conversion assay; Surgery outcome; α-synuclein.
© 2022. The Author(s).
Conflict of interest statement
GG reports no disclosures. SB reports no disclosures. SD reports no disclosures. CZ reports no disclosures. SC reports no disclosures. ND reports no disclosures. HKJ reports no disclosures. MR reports no disclosures. BP reports no disclosures. CQ reports no disclosures. CS reports no disclosures. PC reports no disclosures. DM reports no disclosures. SKH reports no disclosures. GP reports no disclosures. VL reports no disclosers. PP reports no disclosures.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
