

External validation of models for predicting risk of colorectal cancer using the China Kadoorie Biobank
- PMID: 36071519
- PMCID: PMC9454206
- DOI: 10.1186/s12916-022-02488-w
External validation of models for predicting risk of colorectal cancer using the China Kadoorie Biobank
Abstract
Background: In China, colorectal cancer (CRC) incidence and mortality have been steadily increasing over the last decades. Risk models to predict incident CRC have been developed in various populations, but they have not been systematically externally validated in a Chinese population. This study aimed to assess the performance of risk scores in predicting CRC using the China Kadoorie Biobank (CKB), one of the largest and geographically diverse prospective cohort studies in China.
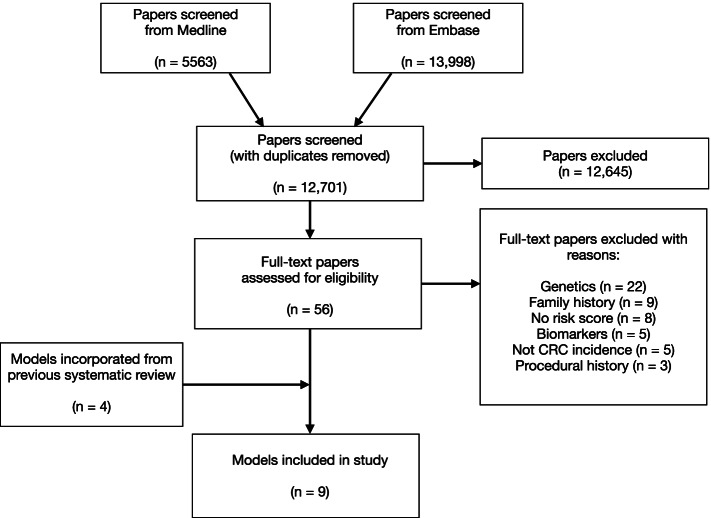
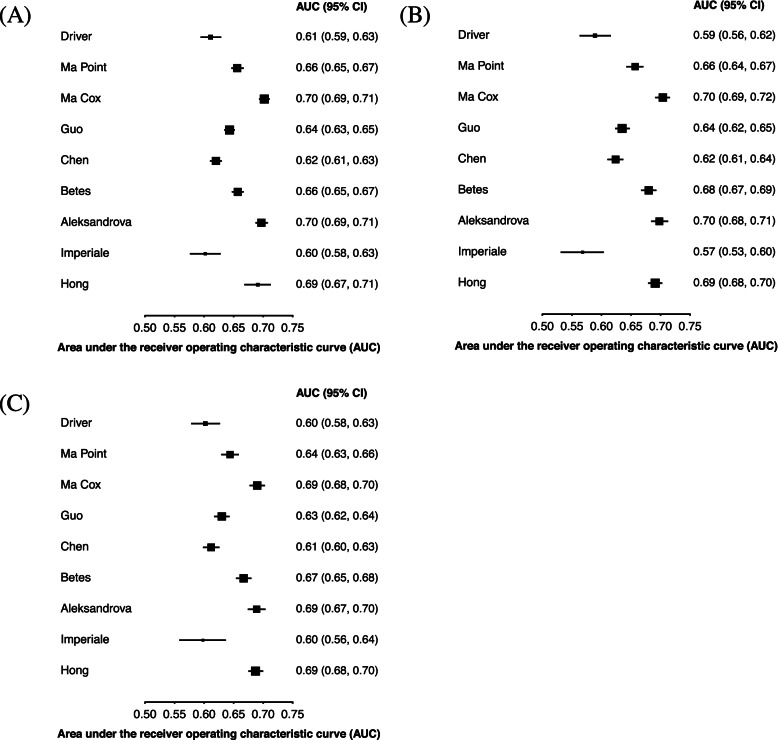
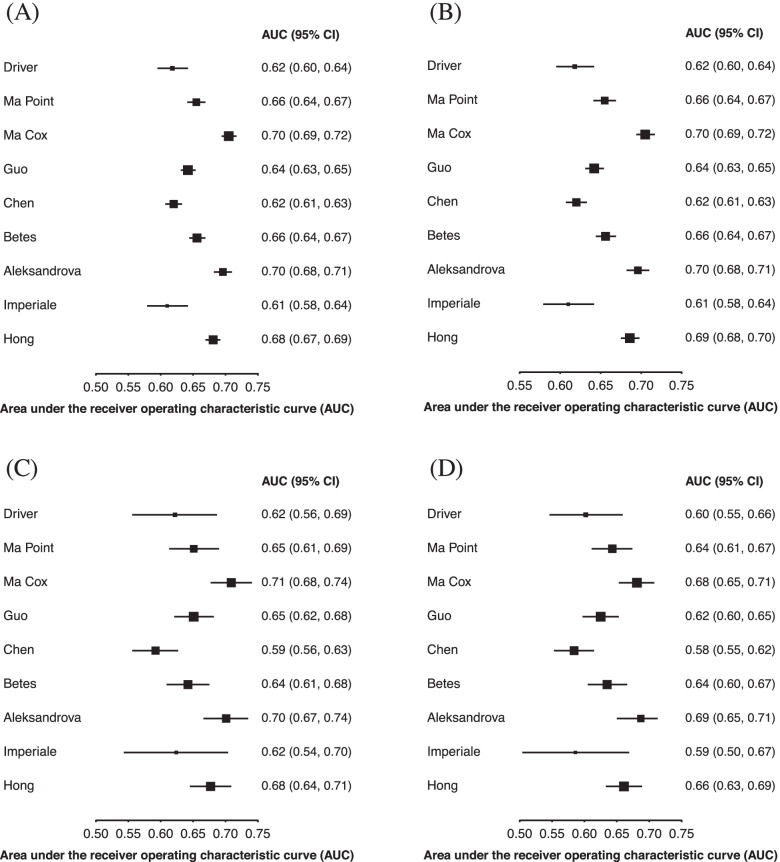
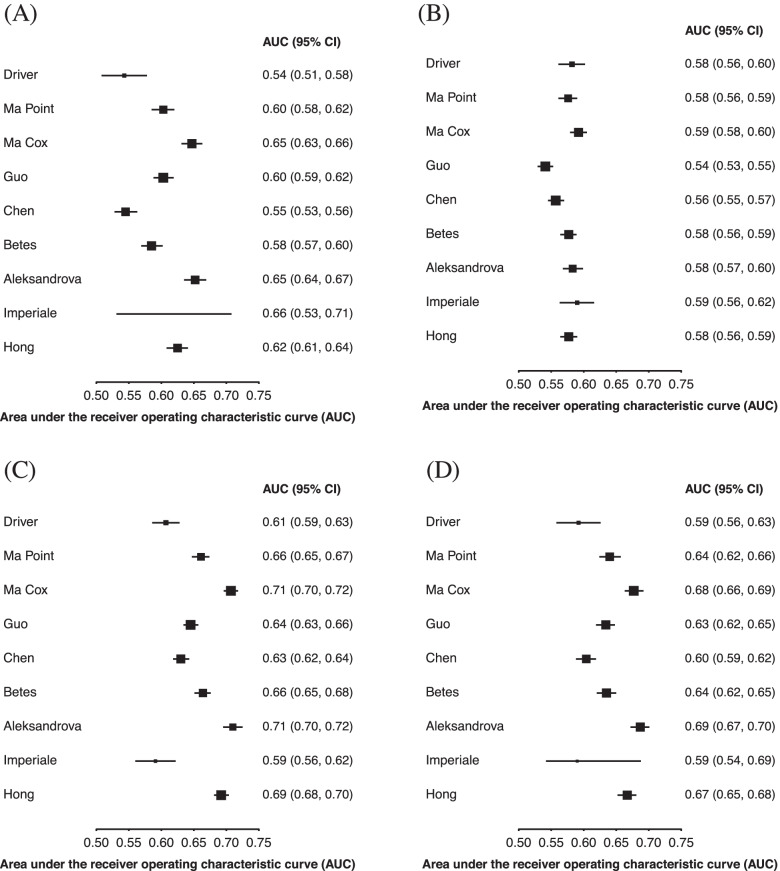
Methods: Nine models were externally validated in 512,415 participants in CKB and included 2976 cases of CRC. Model discrimination was assessed, overall and by sex, age, site, and geographic location, using the area under the receiver operating characteristic curve (AUC). Model discrimination of these nine models was compared to a model using age alone. Calibration was assessed for five models, and they were re-calibrated in CKB.
Results: The three models with the highest discrimination (Ma (Cox model) AUC 0.70 [95% CI 0.69-0.71]; Aleksandrova 0.70 [0.69-0.71]; Hong 0.69 [0.67-0.71]) included the variables age, smoking, and alcohol. These models performed significantly better than using a model based on age alone (AUC of 0.65 [95% CI 0.64-0.66]). Model discrimination was generally higher in younger participants, males, urban environments, and for colon cancer. The two models (Guo and Chen) developed in Chinese populations did not perform better than the others. Among the 10% of participants with the highest risk, the three best performing models identified 24-26% of participants that went on to develop CRC.
Conclusions: Several risk models based on easily obtainable demographic and modifiable lifestyle factor have good discrimination in a Chinese population. The three best performing models have a higher discrimination than using a model based on age alone.
Keywords: Cancer epidemiology; Colorectal cancer; External validation; Risk prediction models.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- England PH. Bowel cancer screening: programme overview GOV.UK2021 [Available from: https://www.gov.uk/guidance/bowel-cancer-screening-programme-overview#ta....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
