

Mannitol Anaphylaxis in the Setting of Septic Emboli-Induced Intracranial Hemorrhage
- PMID: 36072212
- PMCID: PMC9440351
- DOI: 10.7759/cureus.27665
Mannitol Anaphylaxis in the Setting of Septic Emboli-Induced Intracranial Hemorrhage
Abstract
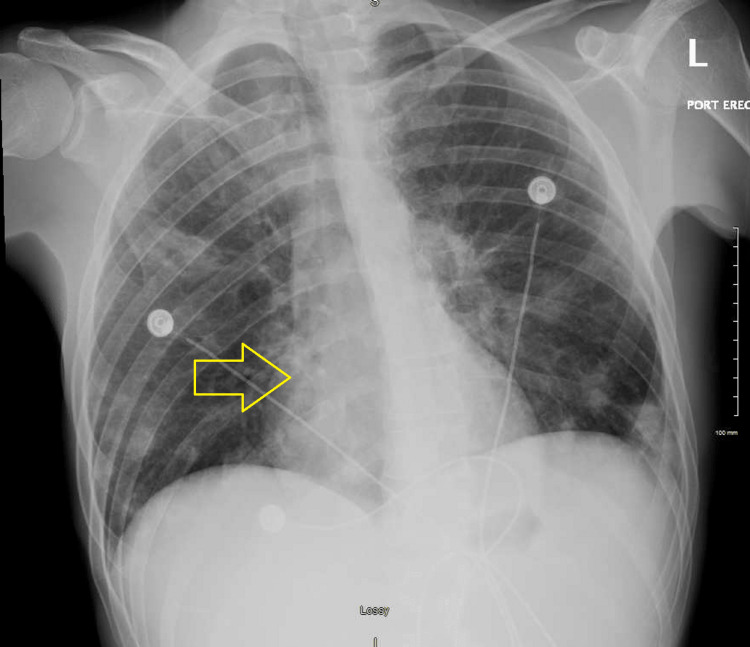
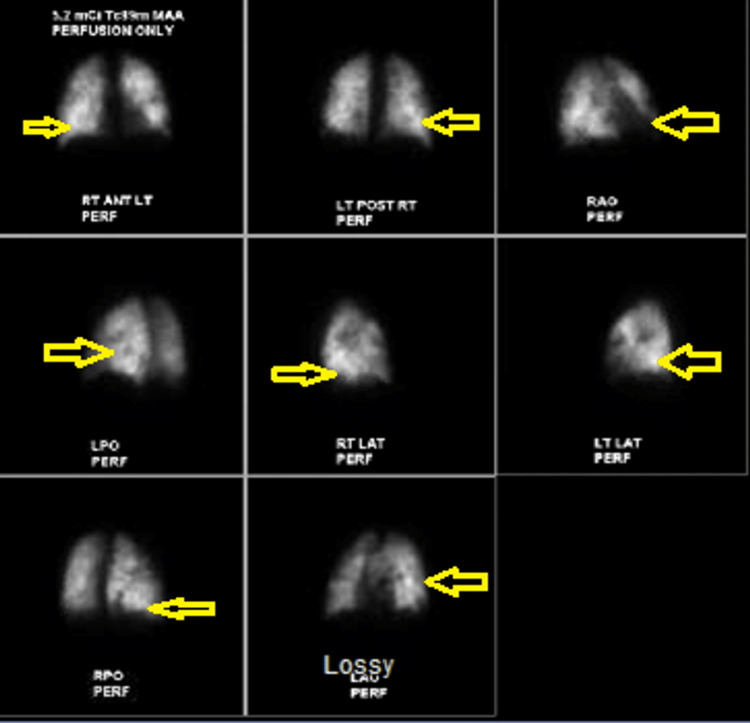
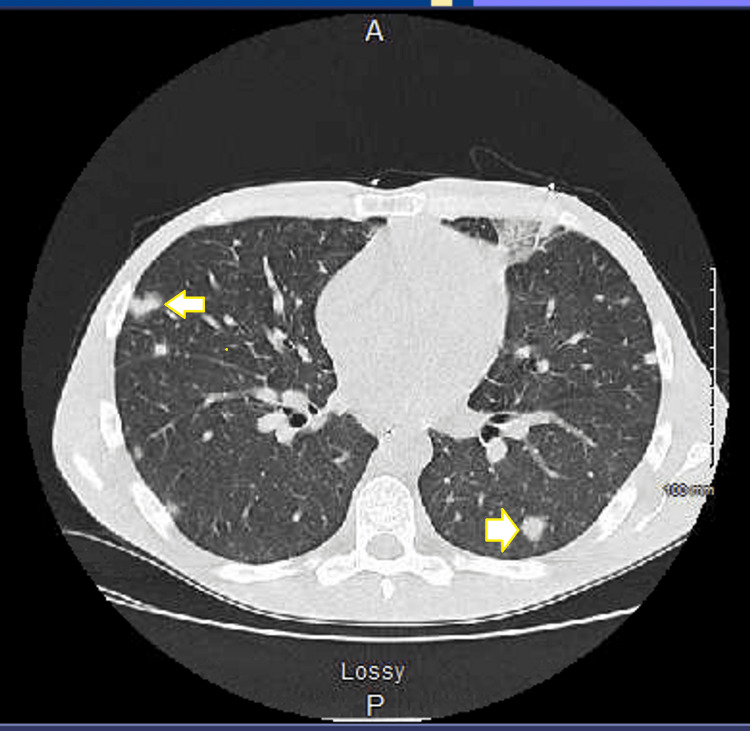
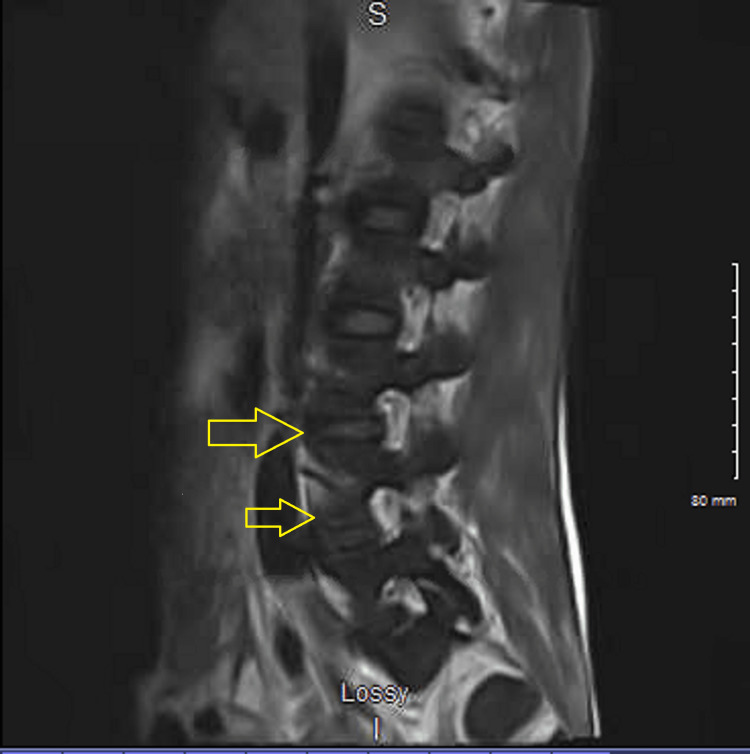
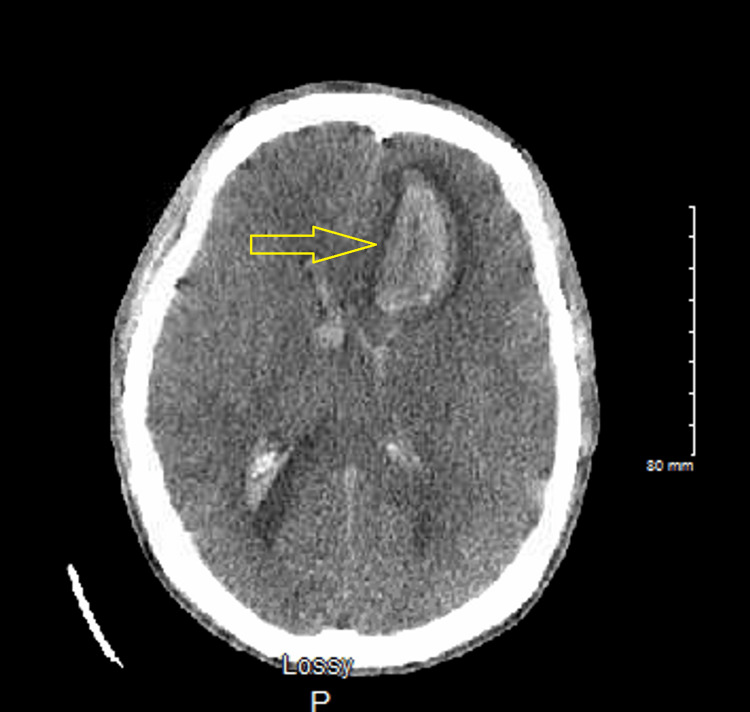
Neurological complications are a significant problem in bacterial endocarditis. Cerebral embolism is the most frequent concern. Acute embolic disease may trigger focal seizures or mycotic aneurysms. Miliary infection is also common, and lumbar puncture can guide in determining the infective organism. Purulent cerebrospinal fluid (CSF) consists often of Staphylococcus aureus, a virulent organism, whereas non-virulent organisms (i.e., viridans streptococci) have normal CSF formulae. Microscopic abscesses suggest the potential for aneurysm from bacterial endocarditis amplifying the risk of intracranial hemorrhage. Mannitol and hypertonic (3%) saline are intravenous medications used as a rescue treatment for brain hemorrhage. A patient diagnosed with mycoplasma pneumonia and septic shock secondary to tricuspid endocarditis with extensive pulmonary emboli and metastatic infection to his spine was initiated on antibiotics. He developed a massive intracranial bleed from the rupture of mycotic septic emboli and was given mannitol to decrease intracranial pressure, which caused anaphylaxis.
Keywords: allergic reaction; allergy and anaphylaxis; bacterial endocarditis; septic emboli; spontaneous intracranial hemorrhage.
Copyright © 2022, Parker et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Bacterial endocarditis and cerebrovascular disease. Silver B, Behrouz R, Silliman S. Curr Neurol Neurosci Rep. 2016;16:104. - PubMed
-
- Evidence for mannitol as an effective agent against intracranial hypertension: an individual patient data meta-analysis. Poole D, Citerio G, Helbok R, et al. Neurocrit Care. 2020;32:252–261. - PubMed
-
- Hypertonic saline for increased intracranial pressure after aneurysmal subarachnoid hemorrhage: a systematic review. Pasarikovski CR, Alotaibi NM, Al-Mufti F, Macdonald RL. World Neurosurg. 2017;105:1–6. - PubMed
-
- Treatment of elevated intracranial pressure in experimental intracerebral hemorrhage: comparison between mannitol and hypertonic saline. Qureshi AI, Wilson DA, Traystman RJ. Neurosurgery. 1999;44:1055–1063. - PubMed
Publication types
LinkOut - more resources
Full Text Sources