

Prognosis of PCI in AMI setting in the elderly population: Outcomes from the multicenter prospective e-ULTIMASTER registry
- PMID: 36072999
- PMCID: PMC9748751
- DOI: 10.1002/clc.23902
Prognosis of PCI in AMI setting in the elderly population: Outcomes from the multicenter prospective e-ULTIMASTER registry
Abstract
Background: Elderly patients with ST-elevation myocardial infarction (STEMI) who undergo percutaneous coronary intervention (PCI) are usually excluded from major trials.
Hyopthesis: This study sought to assess 1-year clinical outcomes following PCI with a drug-eluting stent in patients older than 80 years old with STEMI.
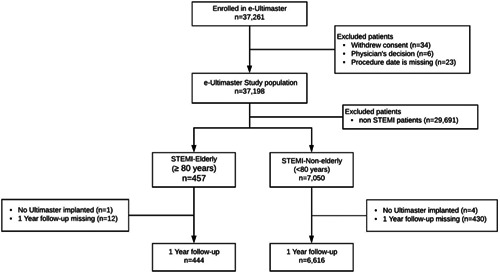
Methods: The large all-comer, multicontinental e-ULTIMASTER registry included 7507 patients with STEMI who underwent PCI using the Ultimaster stent. The primary clinical endpoint was 1-year target lesion failure, a composite of cardiac death (CD), target vessel-related myocardial infarction (TV-MI), or clinically driven target lesion revascularization (CD-TLR).
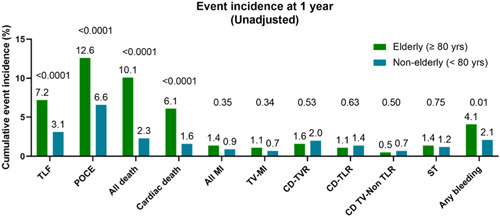
Results: There were 457 (6.1%) patients in the elderly group (≥80 years old) that were compared to 7050 (93.9%) patients <80 years. The elderly patients included more female patients and had significantly more comorbidities and had more complex coronary anatomy. The primary endpoint occurred in 7.2% of the elderly, compared to 3.1% of the younger group (p < .001). All-cause mortality was significantly higher among the elderly group compared to the younger group (10.1% vs. 2.3%, p < .0001), as well as CD (6.1% vs. 1.6%, p < .0001), but not TV-MI (1.1% vs. 0.7%, p = .34) or CD-TLR (1.1% vs. 1.4%, p = .63).
Conclusion: Elderly patients with STEMI presentation had a higher incidence of the composite endpoint than younger patients. All-cause and CD were higher for elderly patients compared to patients younger than 80 years old. However, there was no difference in the incidence of TV-MI or target lesion revascularizations. These findings suggest that PCI for STEMI in elderly patients is relatively safe.
Keywords: age; coronary artery disease; elderly; myocardial infarction; outcome; stent.
© 2022 The Authors. Clinical Cardiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Morici N, De Servi S, De Luca L, et al. Management of acute coronary syndromes in older adults. Eur Heart J. 2022;43:1542‐1553. - PubMed
-
- Renilla A, Barreiro M, Barriales V, Torres F, Alvarez P, Lambert JL. Management and risk factors for mortality in very elderly patients with acute myocardial infarction. Geriatr Gerontol Int. 2013;13:146‐151. - PubMed
-
- Sawant AC, Josey K, Plomondon ME, et al. Temporal trends, complications, and predictors of outcomes among nonagenarians undergoing percutaneous coronary intervention: insights from the veterans affairs clinical assessment, reporting, and tracking program. JACC Cardiovasc Interv. 2017;10:1295‐1303. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
