

Can Technology Assistance be Cost Effective in TKA? A Simulation-Based Analysis of a Risk-prioritized, Practice-specific Framework
- PMID: 36073992
- PMCID: PMC9750678
- DOI: 10.1097/CORR.0000000000002375
Can Technology Assistance be Cost Effective in TKA? A Simulation-Based Analysis of a Risk-prioritized, Practice-specific Framework
Abstract
Background: Robotic, navigated, and patient-specific instrumentation (PSI) TKA procedures have been introduced to improve component placement precision and improve implant survivorship and other clinical outcomes. However, the best available evidence has shown that these technologies are ineffective in reducing revision rates in the general TKA patient population. Nonetheless, it seems plausible that these technologies could be an effective and cost-effective means of reducing revision risk in clinical populations that are at an elevated risk of revision because of patient-specific demographics (such as older age at index surgery, elevated BMI, and being a man). Since clinical trials on this topic would need to be very large, a simulation approach could provide insight on which clinical populations would be the most promising for analysis.
Questions/purposes: We conducted a simulation-based analysis and asked: (1) Given key demographic parameters characterizing a patient population, together with estimates of the precision achievable with selected forms of technology assistance in TKA, can we estimate the expected distributions of anticipated reductions in lifetime revision risk for that population and the associated improvements in quality-adjusted life years (QALYs) that would be expected to result? (2) Are there realistic practice characteristics (such as combinations of local patient demographics and capital and per-procedure costs) for which applying a per-patient risk-prioritized policy for using technology-assisted TKA could be considered cost-effective based on projected cost savings from reductions in revision rates?
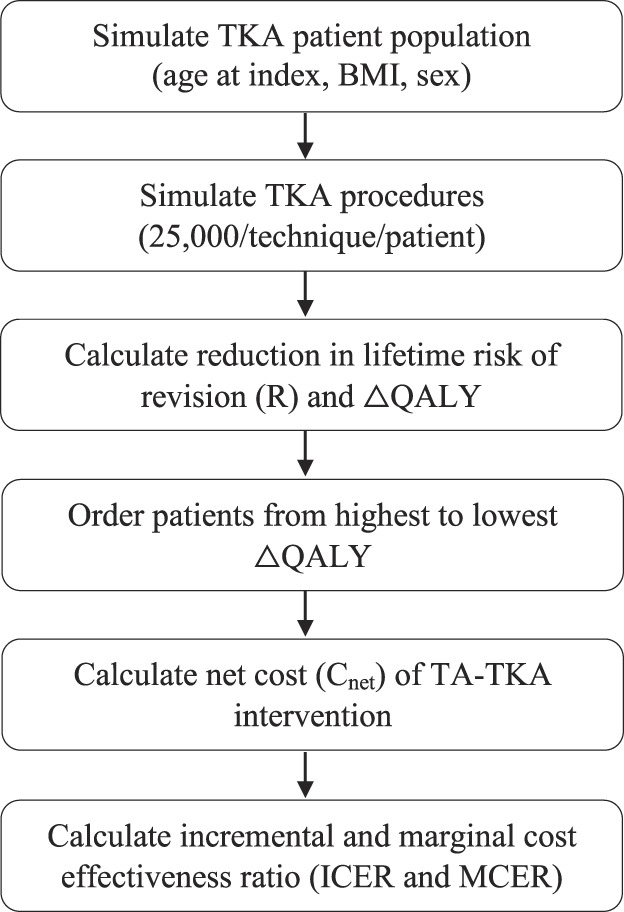
Methods: We designed simulations of hypothetical practice-specific clinical scenarios, each characterized by patient volume, patient demographics, and technology-assisted surgical technique, using demographic information drawn from other studies to characterize two contrasting simulated clinical scenarios in which the distributions of factors describing patients undergoing TKA place one population at a comparatively elevated risk of revision (elevated-risk population) and the second at a comparatively reduced risk of revision (lower-risk population). We used results from previous systematic reviews and meta-analyses to estimate the implant precision in coronal plane alignment for patient-specific instrumentation, navigated, and robotic technology. We generated simulated TKA patient populations based on risk estimates from large clinical studies, structured reviews, and meta-analyses and calculated the patient-specific reduction in the revision risk and the change in QALYs attributable to the technology-assisted intervention in each of the two simulated clinical scenarios. We also incorporated a sensitivity analysis, incorporating variations in the effect size of deviations from overall coronal alignment on revision risk and difference in health state utilities acquired through a structured review process. We then simulated the outcomes of 25,000 operations per patient using the precisions associated with the conventional TKA technique, the three technology-assisted techniques, and a hypothetical technology-assisted intervention that could consistently deliver perfectly neutral overall coronal alignment, which is unachievable in practice. A risk-prioritized treatment policy was emulated by ordering the simulated patients from the highest to lowest predicted increase in QALYs, such that simulated patients who would see the greatest increase in the QALYs (and therefore the greatest reduction in lifetime revision risk) were the patients to receive technology-assisted TKA intervention in a practice. We used cost estimates acquired through a structured review process and calculated the net added costs of each of the three technology-assisted techniques as a function of the percent utilization (proportion of patients treated with technology assistance in a practice), factoring in fixed costs, per-procedure variable costs, and savings occurring from the prevention of future revision surgery. Finally, we calculated the incremental cost-effectiveness ratio (ICER) and marginal cost-effectiveness ratio (MCER) for each technology-assisted technique for the two clinical scenarios. We then used a Monte Carlo approach to simulate variations in key patient risk, health state, and economic factors as well as to obtain a distribution of estimates for cost-effectiveness. We considered an intervention to be cost effective if either the ICER or MCER values were below USD/QALY 63,000.
Results: For the lower-risk population, the median reduction in the revision risk was 0.9% (0.4% to 2.2%, extrema from the sensitivity analysis) and 1.8% (0.9% to 4.4%) for PSI and robotic TKA, respectively, and 1.9% (1.0% to 4.6%) for ideal TKA. In contrast, the median reduction in the revision risk in the elevated-risk clinical scenario was 2.0% (1.2% to 3.4%) and 4.6% (2.7% to 8.5%) for PSI and robotic TKA and 5.1% (3.0% to 9.4%) for ideal TKA. Estimated differences in the cumulative gain in QALYs attributable to technology-assisted TKA ranged from 0.6 (0.2 to 1.8) to 4.0 (1.8 to 10.0) QALYs per 100 patients, depending on the intervention type and clinical scenario. For PSI, we found treating 15% of patients in the lower-risk population and 77% in the elevated-risk population could meet the threshold for being considered cost effective. For navigated TKA systems offering high alignment precision, we found the intervention could meet this threshold for practice sizes of at least 300 patients per year and a percent utilization of 27% in the lower-risk population. In the elevated-risk population, cost-effectiveness could be achieved in practice volumes as small as 100 patients per year with a percent utilization of at least 6%, and cost savings could be achieved with a percent utilization of at least 45%. We found that robotic TKA could only meet the threshold for being considered cost-effectiveness in the lower-risk population if yearly patient volumes exceeded 600 and for a limited range of percent utilization (27% to 32%). However, in the elevated-risk patient population, robotic TKA with high alignment precision could potentially be cost effective for practice sizes as small as 100 patients per year and a percent utilization of at least 20% if a risk-prioritized treatment protocol were used.
Conclusion: Based on these simulations, a selective-use policy for technology-assisted TKA that prioritizes using technology assistance for those patients at a higher risk of revision based on patient-specific factors could potentially meet the cost-effectiveness threshold in selected circumstances (for example, primarily in elevated-risk populations and larger practice sizes). Whether it does meet that threshold would depend significantly on the surgical precision that can be achieved in practice for a given proposed technology as well as on the true local costs of using the proposed technology. We further recommend that any future randomized trials seeking to demonstrate possible effects of technology assistance on revision risk focus on clinical populations that are at higher risk of revision (such as, patient populations that are relatively younger, have higher BMIs, and higher proportions of men).
Clinical relevance: This study suggests that technology assistance is only likely to prove cost effective in selected circumstances rather than in all clinical populations and practice settings. In general, we project that surgical navigation is most likely to prove cost effective in the widest range of circumstances, that PSI may be cost effective or cost neutral in a moderate range of circumstances, and that robotic surgery is only likely to be cost effective in moderately large practices containing patients who are on average at an intrinsically elevated risk of revision.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures







Comment in
-
CORR Insights®: Can Technology Assistance be Cost Effective in TKA? A Simulation-based Analysis of a Risk-prioritized, Practice-specific Framework.Clin Orthop Relat Res. 2023 Jan 1;481(1):174-176. doi: 10.1097/CORR.0000000000002426. Epub 2022 Sep 27. Clin Orthop Relat Res. 2023. PMID: 36170156 Free PMC article. No abstract available.
References
-
- American Academy of Orthopaedic Surgeons. American Joint Replacement Registry 2021 Annual Report. Available at: https://connect.registryapps.net/2021-ajrr-annual-report. Accessed January 10, 2022.
-
- Barrack RL, Ruh EL, Williams BM, Ford AD, Foreman K, Nunley RM. Patient specific cutting blocks are currently of no proven value. J Bone Joint Surg Br. 2012;94:95-99. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
