

Preclinical and Clinical Efficacy of Trastuzumab Deruxtecan in Breast Cancer Brain Metastases
- PMID: 36074155
- PMCID: PMC9811155
- DOI: 10.1158/1078-0432.CCR-22-1138
Preclinical and Clinical Efficacy of Trastuzumab Deruxtecan in Breast Cancer Brain Metastases
Abstract
Purpose: Brain metastases can occur in up to 50% of patients with metastatic HER2-positive breast cancer. Because patients with active brain metastases were excluded from previous pivotal clinical trials, the central nervous system (CNS) activity of the antibody-drug conjugate trastuzumab deruxtecan (T-DXd) is not well characterized.
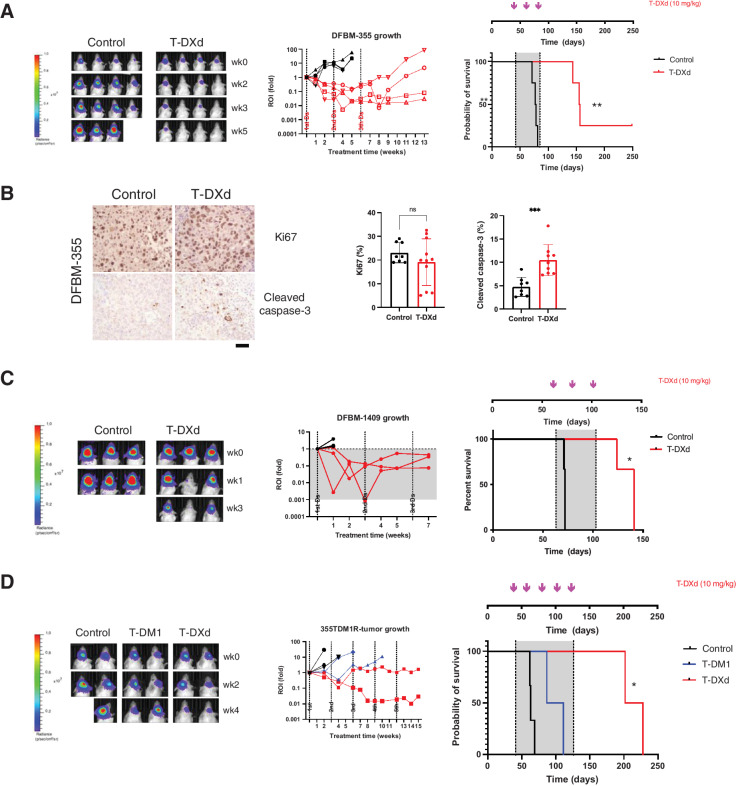
Experimental design: We studied how T-DXd affects growth and overall survival in orthotopic patient-derived xenografts (PDX) of HER2-positive and HER2-low breast cancer brain metastases (BCBM). Separately, we evaluated the effects of T-DXd in a retrospective cohort study of 17 patients with stable or active brain metastases.
Results: T-DXd inhibited tumor growth and prolonged survival in orthotopic PDX models of HER2-positive (IHC 3+) and HER2-low (IHC 2+/FISH ratio < 2) BCBMs. T-DXd reduced tumor size and prolonged survival in a T-DM1-resistant HER2-positive BCBM PDX model. In a retrospective multi-institutional cohort study of 17 patients with predominantly HER2-positive BCBMs, the CNS objective response rate (ORR) was 73% (11/15) while extracranial response rate was 45% (5/11). In the subset of patients with untreated or progressive BCBM at baseline, the CNS ORR was 70% (7/10). The median time on treatment with T-DXd was 8.9 (1.3-16.2) months, with 42% (7/17) remaining on treatment at data cutoff.
Conclusions: T-DXd demonstrates evidence of CNS activity in HER2-positive and HER2-low PDX models of BCBM and preliminary evidence of clinical efficacy in a multi-institution case series of patients with BCBM. Prospective clinical trials to further evaluate CNS activity of T-DXd in patients with active brain metastases are warranted. See related commentary by Soffietti and Pellerino, p. 8.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures

Comment in
-
Brain Metastasis from HER2-Positive Breast Cancer: An Evolving Landscape.Clin Cancer Res. 2023 Jan 4;29(1):8-10. doi: 10.1158/1078-0432.CCR-22-2853. Clin Cancer Res. 2023. PMID: 36305867
-
Preclinical and clinical efficacy of trastuzumab-deruxtecan in breast cancer brain metastases: a new insight on central nervous system activity.Ann Transl Med. 2023 Oct 25;11(11):398. doi: 10.21037/atm-23-1603. Epub 2023 Oct 17. Ann Transl Med. 2023. PMID: 37970592 Free PMC article. No abstract available.
Comment on
-
Brain Metastasis from HER2-Positive Breast Cancer: An Evolving Landscape.Clin Cancer Res. 2023 Jan 4;29(1):8-10. doi: 10.1158/1078-0432.CCR-22-2853. Clin Cancer Res. 2023. PMID: 36305867
References
-
- Pestalozzi BC, Holmes E, de Azambuja E, Metzger-Filho O, Hogge L, Scullion M, et al. CNS relapses in patients with HER2-positive early breast cancer who have and have not received adjuvant trastuzumab: a retrospective substudy of the HERA trial (BIG 1-01). Lancet Oncol 2013;14:244–8. - PubMed
-
- Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J Clin Oncol 2018;36:2105–22. - PubMed
-
- Kennecke H, Yerushalmi R, Woods R, Cheang MC, Voduc D, Speers CH, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol 2010;28:3271–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
