

Anti-spike T-cell and Antibody Responses to SARS-CoV-2 mRNA Vaccines in Patients with Hematologic Malignancies
- PMID: 36074641
- PMCID: PMC9894565
- DOI: 10.1158/2643-3230.BCD-22-0077
Anti-spike T-cell and Antibody Responses to SARS-CoV-2 mRNA Vaccines in Patients with Hematologic Malignancies
Abstract
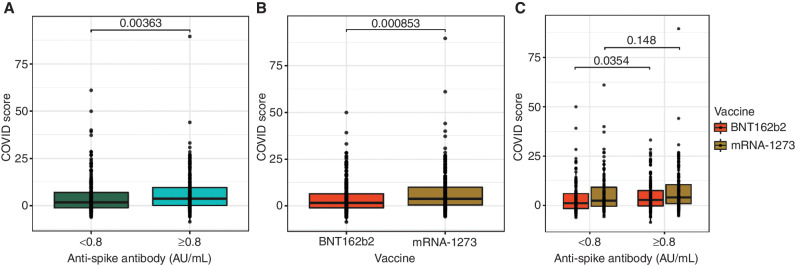
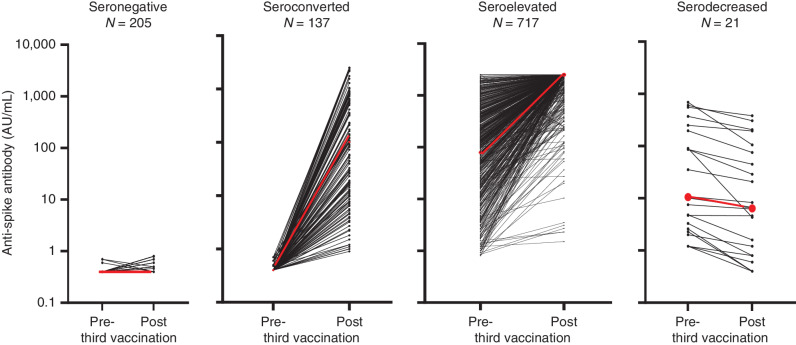
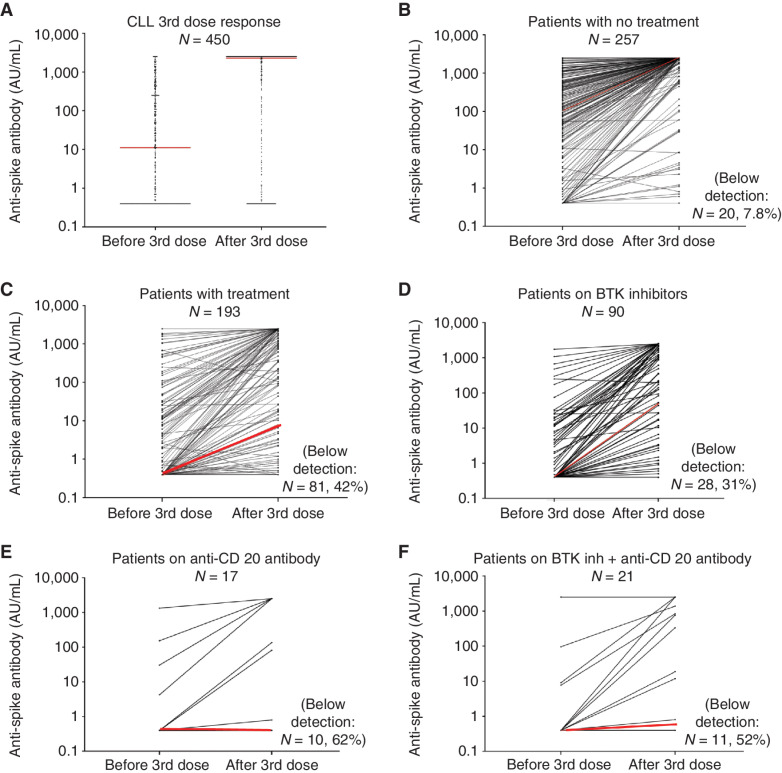
The anti-spike T-cell and antibody responses to SARS-CoV-2 mRNA vaccines in patients with B-cell malignancies were examined in a real-world setting. A next-generation sequencing (NGS)-based molecular assay was used to assess SARS-CoV-2-specific T-cell responses. After the second dose, 58% (166/284) of seropositive and 45% (99/221) of seronegative patients display anti-spike T cells. The percentage of patients who displayed T-cell response was higher among patients receiving mRNA-1273 vaccines compared with those receiving BNT162b2 vaccines. After the third vaccination, 40% (137/342) of patients seroconverted, although only 22% displayed sufficient antibody levels associated with the production of neutralizing antibodies. 97% (717/738) of patients who were seropositive before the third dose had markedly elevated anti-spike antibody levels. Anti-spike antibody levels, but not T-cell responses, were depressed by B cell-directed therapies. Vaccinated patients with B-cell malignancies with a poor response to SARS-CoV-2 vaccines may remain vulnerable to COVID-19 infections.
Significance: This study represents the first investigation of SARS-CoV-2-specific immune responses to vaccination in a patient registry using an NGS-based method for T-cell receptor repertoire-based analysis combined with anti-spike antibody assessments. Vaccinated patients with B cell-derived hematologic malignancies are likely at higher risk of infection or severe COVID-19. This article is highlighted in the In This Issue feature, p. 476.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Khoury DS, Cromer D, Reynaldi A, Schlub TE, Wheatley AK, Juno JA, et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med 2021;7:1205–11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
