

Orthopoxvirus Testing Challenges for Persons in Populations at Low Risk or Without Known Epidemiologic Link to Monkeypox - United States, 2022
- PMID: 36074752
- PMCID: PMC9470221
- DOI: 10.15585/mmwr.mm7136e1
Orthopoxvirus Testing Challenges for Persons in Populations at Low Risk or Without Known Epidemiologic Link to Monkeypox - United States, 2022
Abstract
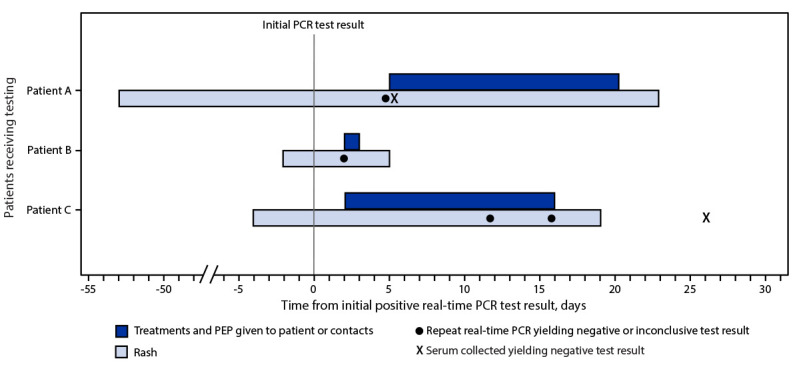
Since May 2022, approximately 20,000 cases of monkeypox have been identified in the United States, part of a global outbreak occurring in approximately 90 countries and currently affecting primarily gay, bisexual, and other men who have sex with men (MSM) (1). Monkeypox virus (MPXV) spreads from person to person through close, prolonged contact; a small number of cases have occurred in populations who are not MSM (e.g., women and children), and testing is recommended for persons who meet the suspected case definition* (1). CDC previously developed five real-time polymerase chain reaction (PCR) assays for detection of orthopoxviruses from lesion specimens (2,3). CDC was granted 510(k) clearance for the nonvariola-orthopoxvirus (NVO)-specific PCR assay by the Food and Drug Administration. This assay was implemented within the Laboratory Response Network (LRN) in the early 2000s and became critical for early detection of MPXV and implementation of public health action in previous travel-associated cases as well as during the current outbreak (4-7). PCR assays (NVO and other Orthopoxvirus laboratory developed tests [LDT]) represent the primary tool for monkeypox diagnosis. These tests are highly sensitive, and cross-contamination from other MPXV specimens being processed, tested, or both alongside negative specimens can occasionally lead to false-positive results. This report describes three patients who had atypical rashes and no epidemiologic link to a monkeypox case or known risk factors; these persons received diagnoses of monkeypox based on late cycle threshold (Ct) values ≥34, which were false-positive test results. The initial diagnoses were followed by administration of antiviral treatment (i.e., tecovirimat) and JYNNEOS vaccine postexposure prophylaxis (PEP) to patients' close contacts. After receiving subsequent testing, none of the three patients was confirmed to have monkeypox. Knowledge gained from these and other cases resulted in changes to CDC guidance. When testing for monkeypox in specimens from patients without an epidemiologic link or risk factors or who do not meet clinical criteria (or where these are unknown), laboratory scientists should reextract and retest specimens with late Ct values (based on this report, Ct ≥34 is recommended) (8). CDC can be consulted for complex cases including those that appear atypical or questionable cases and can perform additional viral species- and clade-specific PCR testing and antiorthopoxvirus serologic testing.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Brian Pope reports travel support and provision of laboratory equipment from the Association for Public Health Laboratories and unpaid participation for service on the Awards and Nominations Committee for the Pan American Society for Clinical virology. Heba H. Mostafa reports grant support from the Maryland Department of Health, and research contract support from BioRad, DiaSorin, and Hologic. No other potential conflicts of interest were disclosed.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
