

Sinus Tachycardia: a Multidisciplinary Expert Focused Review
- PMID: 36074973
- PMCID: PMC9523592
- DOI: 10.1161/CIRCEP.121.007960
Sinus Tachycardia: a Multidisciplinary Expert Focused Review
Abstract
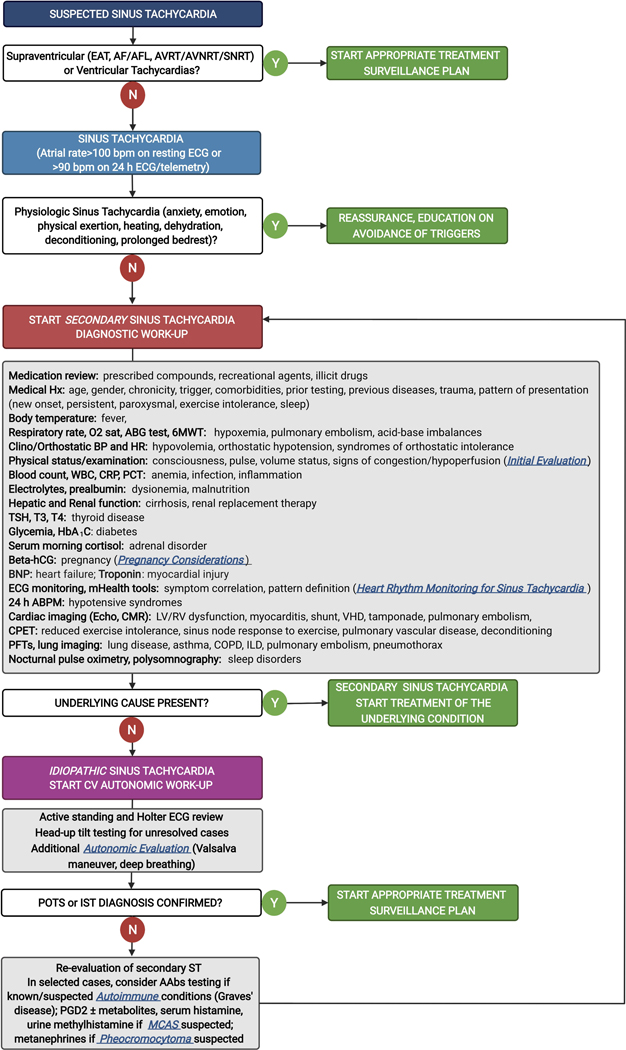
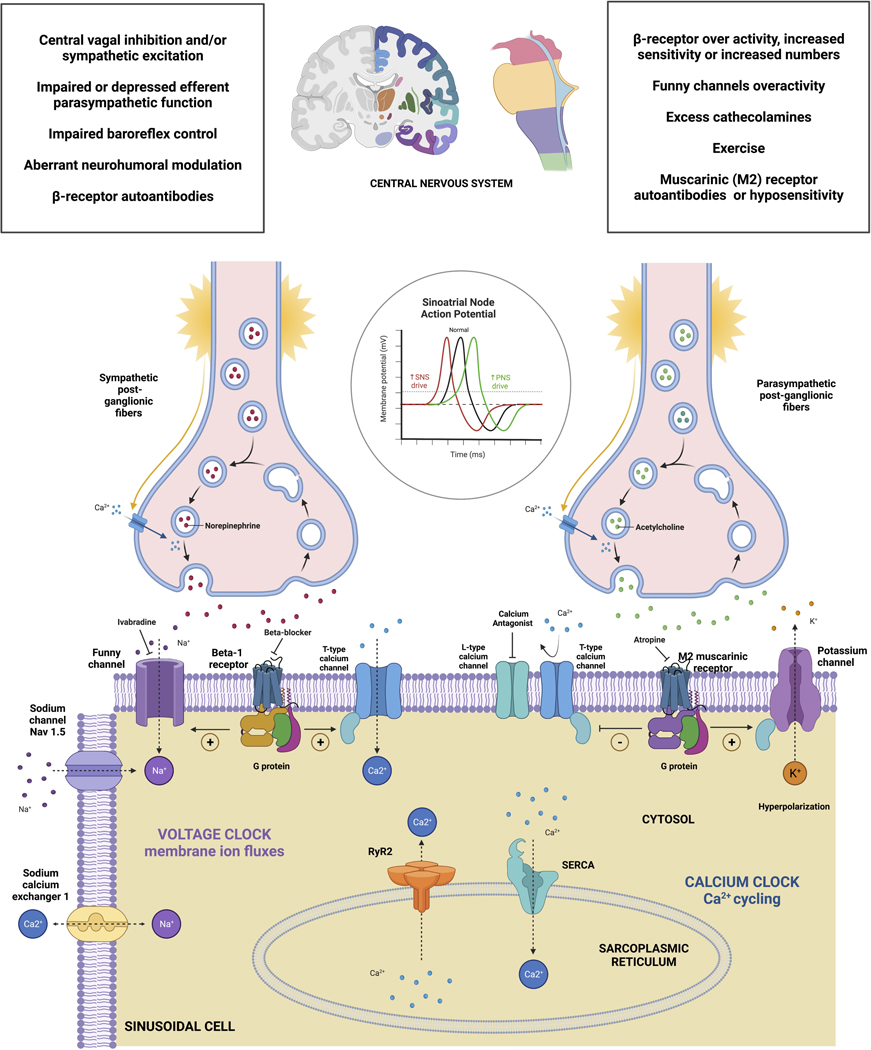
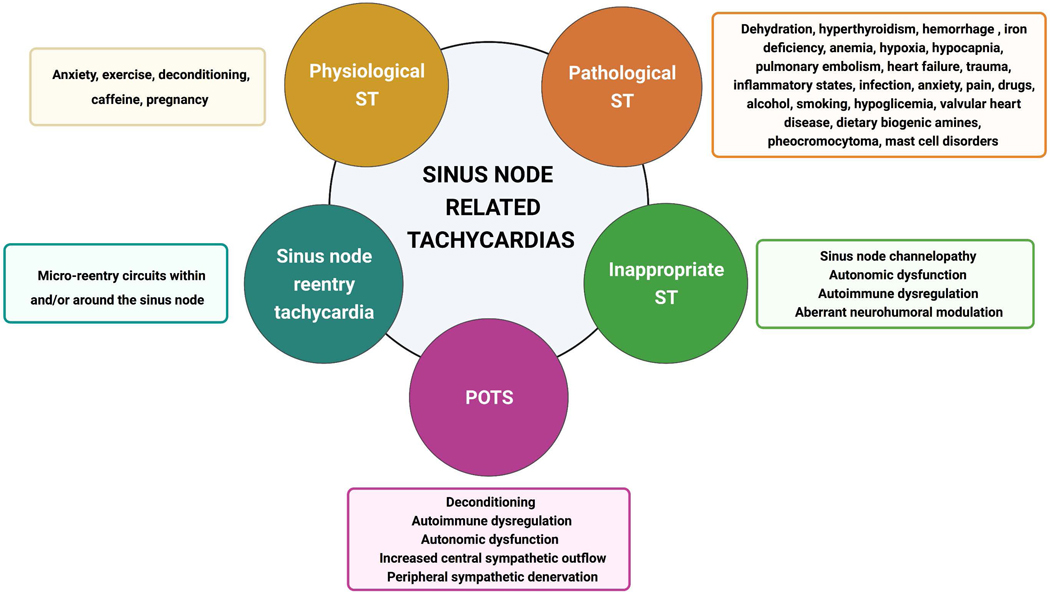
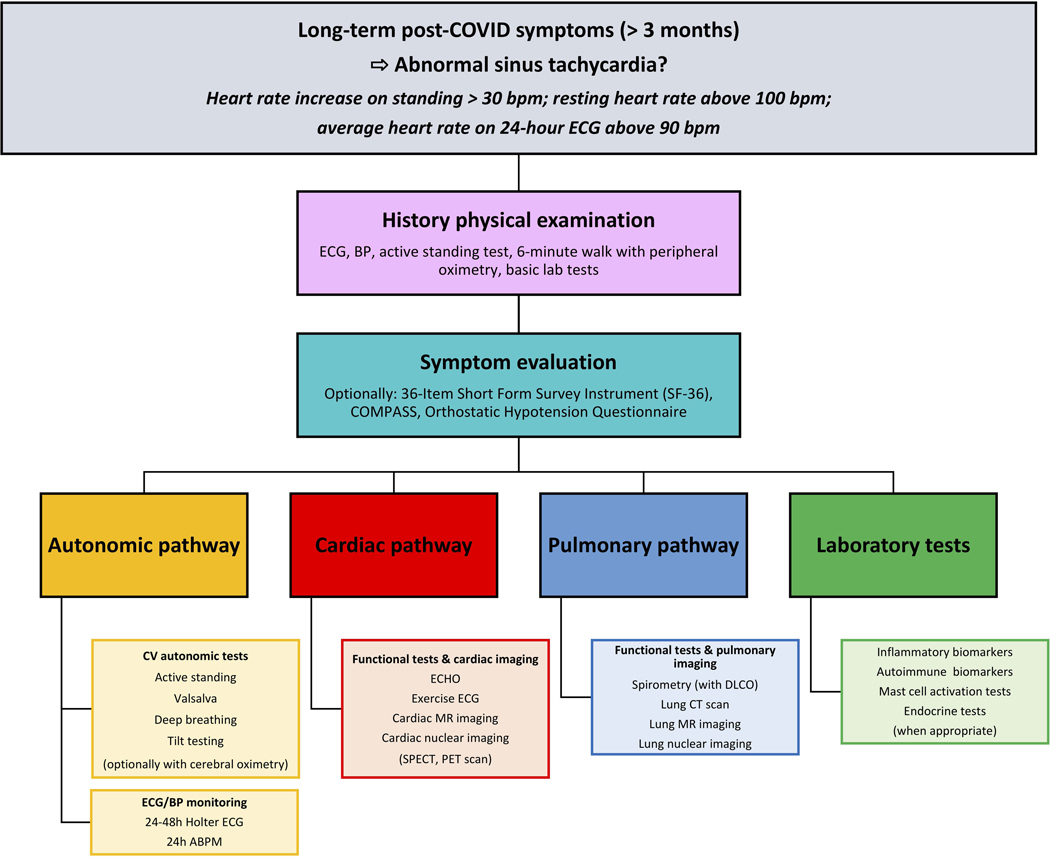
Sinus tachycardia (ST) is ubiquitous, but its presence outside of normal physiological triggers in otherwise healthy individuals remains a commonly encountered phenomenon in medical practice. In many cases, ST can be readily explained by a current medical condition that precipitates an increase in the sinus rate, but ST at rest without physiological triggers may also represent a spectrum of normal. In other cases, ST may not have an easily explainable cause but may represent serious underlying pathology and can be associated with intolerable symptoms. The classification of ST, consideration of possible etiologies, as well as the decisions of when and how to intervene can be difficult. ST can be classified as secondary to a specific, usually treatable, medical condition (eg, pulmonary embolism, anemia, infection, or hyperthyroidism) or be related to several incompletely defined conditions (eg, inappropriate ST, postural tachycardia syndrome, mast cell disorder, or post-COVID syndrome). While cardiologists and cardiac electrophysiologists often evaluate patients with symptoms associated with persistent or paroxysmal ST, an optimal approach remains uncertain. Due to the many possible conditions associated with ST, and an overlap in medical specialists who see these patients, the inclusion of experts in different fields is essential for a more comprehensive understanding. This article is unique in that it was composed by international experts in Neurology, Psychology, Autonomic Medicine, Allergy and Immunology, Exercise Physiology, Pulmonology and Critical Care Medicine, Endocrinology, Cardiology, and Cardiac Electrophysiology in the hope that it will facilitate a more complete understanding and thereby result in the better care of patients with ST.
Keywords: autonomic dysfunction; hyperthyroidism; inappropriate sinus tachycardia; post-COVID syndrome; postural orthostatic tachycardia syndrome; sinus tachycardia.
Figures
References
-
- Aune D, Sen A, o’Hartaigh B, Janszky I, Romundstad PR, Tonstad S, Vatten LJ. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality - A systematic review and dose-response meta-analysis of prospective studies. Nutr Metab Cardiovasc Dis. 2017;27:504–517. doi: 10.1016/j.numecd.2017.04.004 - DOI - PubMed
