

Prospective Hemophilia Inhibitor PUP Study reveals distinct antibody signatures during FVIII inhibitor eradication
- PMID: 36074992
- PMCID: PMC10165197
- DOI: 10.1182/bloodadvances.2022007267
Prospective Hemophilia Inhibitor PUP Study reveals distinct antibody signatures during FVIII inhibitor eradication
Abstract
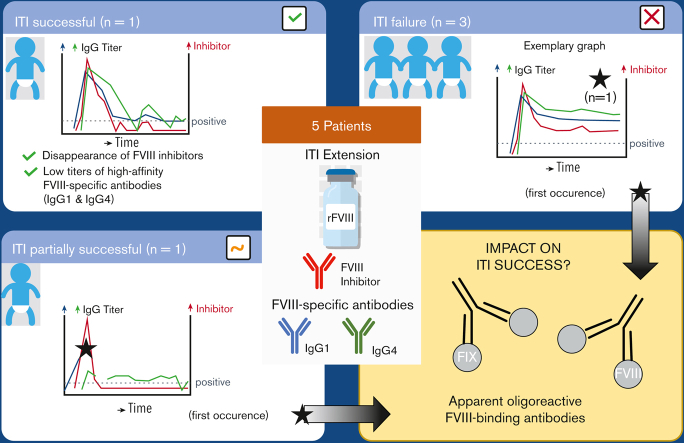
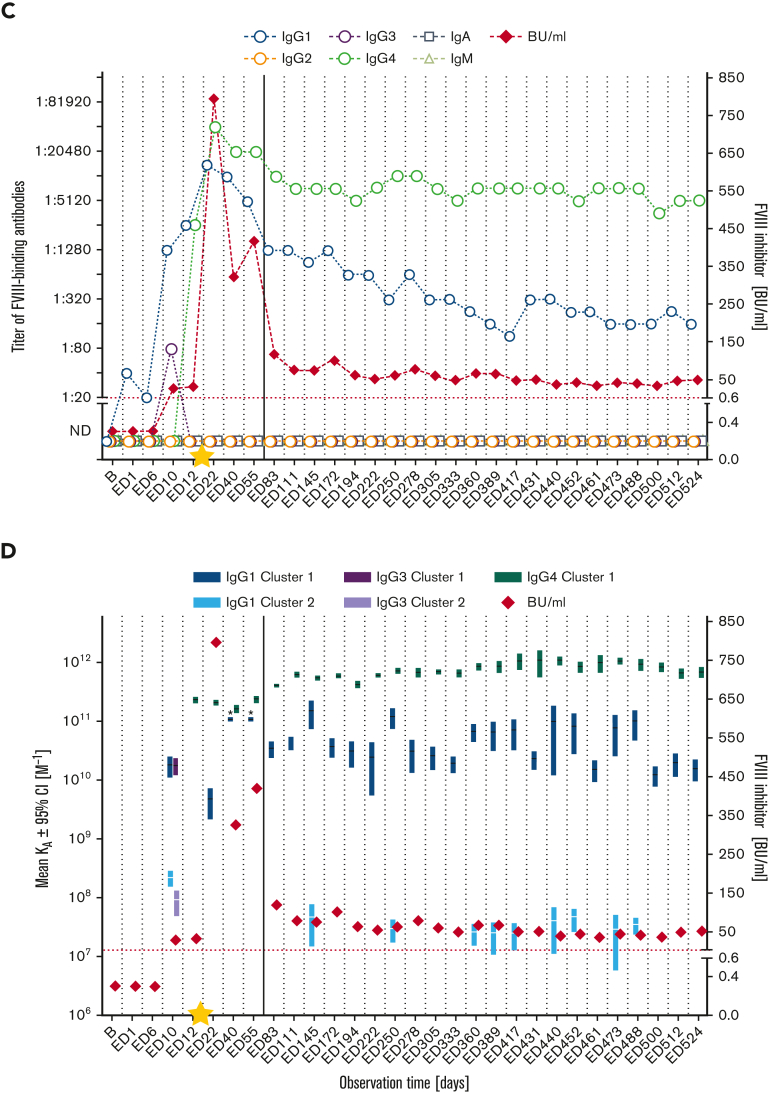
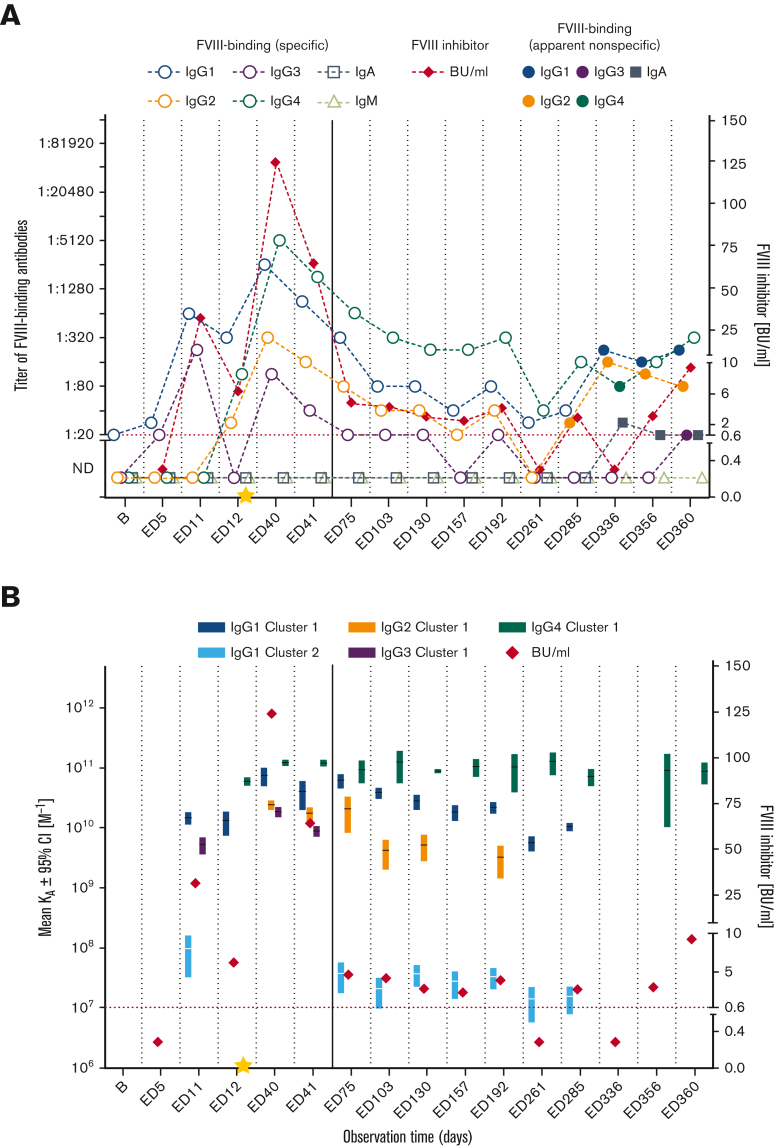
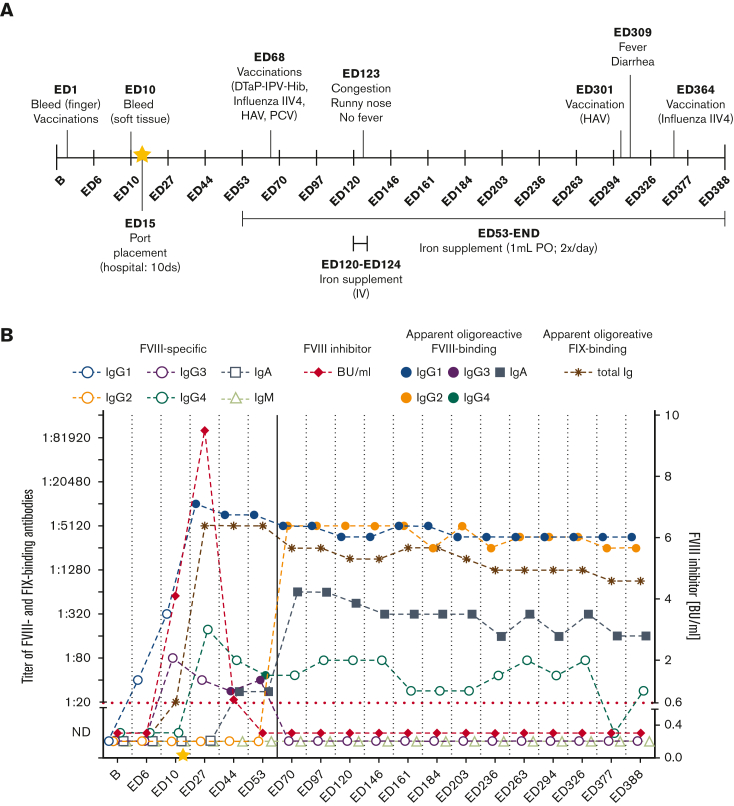
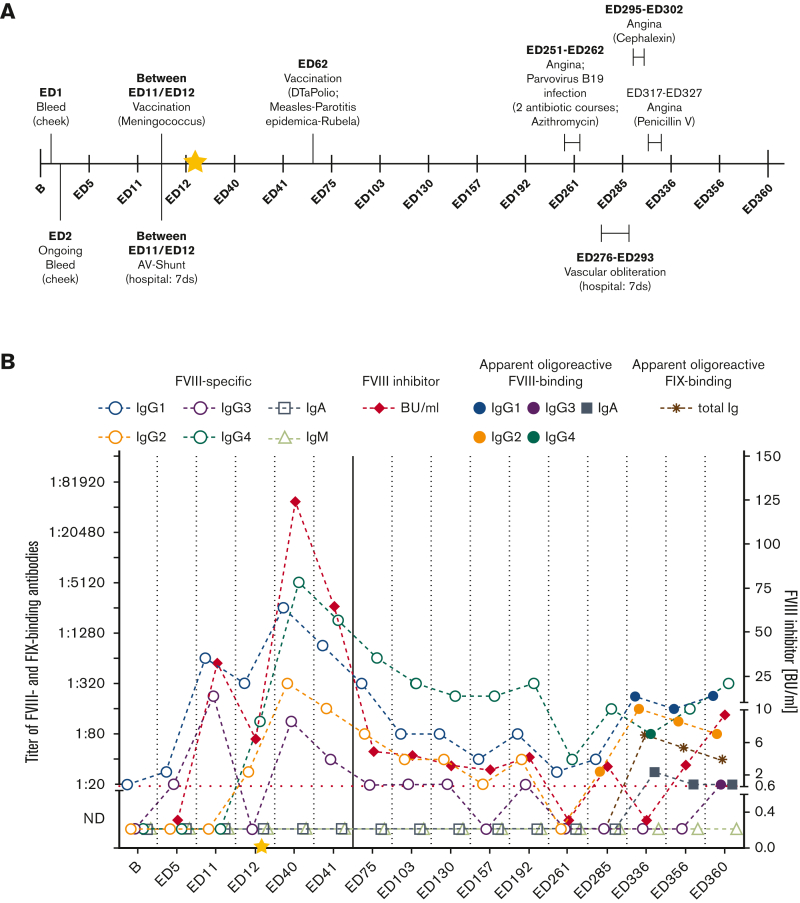
Factor VIII (FVIII) inhibitor formation is a major clinical concern during replacement therapy in patients with hemophilia A. Immune tolerance induction (ITI) is the only therapeutic approach to attempt inhibitor eradication and establishment of long-term immune tolerance to FVIII. Hemophilia Inhibitor Previously Untreated Patient (PUP) Study (HIPS) was a prospective clinical trial to investigate changes in the immune system of PUPs with severe hemophilia A. Five patients who developed persistent FVIII inhibitors during HIPS entered an ITI extension arm (HIPS-ITI). During HIPS-ITI, inhibitor patients received ITI with the same FVIII product (a single source of recombinant, human full-length FVIII) used in HIPS until successful tolerance, declared failure, or a maximum of 2 years after HIPS-ITI enrollment, whichever came first. Blood samples and clinical data were collected monthly. Longitudinal FVIII-binding antibody signatures, associated binding specificities, and apparent affinities were determined for each patient at each sampling time point. ITI was successful or partially successful in 2 patients and failed in 3. Both groups presented with distinct FVIII-specific antibody signatures. ITI success required the disappearance of FVIII inhibitors, which was associated with the eradication or sustained titer minimization of high-affinity FVIII-specific antibodies, particularly of the immunoglobulin G1 (IgG1) and IgG4 subclasses. In contrast, ITI failure, as reflected by FVIII inhibitor persistence, was associated with persistent high-affinity FVIII-specific antibodies. Interestingly, 1 patient with partial ITI success and 1 patient with ITI failure developed apparent oligoreactive FVIII-binding antibodies during ITI. The explanation of the true nature of these antibodies requires more comprehensive follow-ups in future studies. This trial was registered at www.clinicaltrials.gov as #NCT01652027.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: H.P., V.B., and D.L.B. received research funding for institution from Baxalta Innovations GmbH, a Takeda company. B.G. is an employee of Baxalta Innovations GmbH, a Takeda company, and holds stock options of Takeda. J. Bowen received research funding from the study sponsor, University of Texas Health Science Center. P.L. received research funding from the study sponsor, University of Texas Health Science Center, and was an employee of Rho Inc. at the time of the study. J. Blatný received consultation/speakers fee from Takeda, Novo Nordisk, Sobi, LFB, Roche, Pfizer, CSL Behring, and Octapharma. C.M. received fees to institution for study participation from Bayer, Baxalta/Shire/Takeda, Biotest, CSL Behring, Novo Nordisk, and Sobi; unrestricted grant to institution from Biotest and CSL Behring; and personal honoraria (consultancy, speaker, chair) from Bayer, Biotest, CSL Behring, Novo Nordisk, Roche, and Pfizer. V.C.R. received research funding to institution and fees to institution for study participation from Takeda, Pfizer, and Grifols. R.D. was an employee of Baylor College of Medicine at the time of the study. M.E.M. received consultation, advisory, and speaker fees from Bayer, BioMarin, Catalyst Bioscience, CSL Behring, Grifols, Kedrion, LFB, Novo Nordisk, Octapharma, Pfizer, Roche, Sanofi, Sobi, Spark Therapeutics, Takeda, and uniQure. B.M.R. was an employee of Baxalta Innovations GmbH, a Takeda company, at the time of the study.
Figures
References
-
- Gouw SC, van der Bom JG, Ljung R, et al. Factor VIII products and inhibitor development in severe hemophilia A. N Engl J Med. 2013;368(3):231–239. - PubMed
-
- Peyvandi F, Mannucci PM, Garagiola I, et al. A randomized trial of factor VIII and neutralizing antibodies in hemophilia A. N Engl J Med. 2016;374(21):2054–2064. - PubMed
-
- Wight J, Paisley S. The epidemiology of inhibitors in haemophilia A: a systematic review. Haemophilia. 2003;9(4):418–435. - PubMed
-
- Lusher JM, Arkin S, Abildgaard CF, Schwartz RS. Recombinant factor VIII for the treatment of previously untreated patients with hemophilia A. Safety, efficacy, and development of inhibitors. Kogenate Previously Untreated Patient Study Group. N Engl J Med. 1993;328(7):453–459. - PubMed
