

Risk Factors for Heart Failure Among Pan-European Childhood Cancer Survivors: A PanCareSurFup and ProCardio Cohort and Nested Case-Control Study
- PMID: 36075007
- PMCID: PMC9788976
- DOI: 10.1200/JCO.21.02944
Risk Factors for Heart Failure Among Pan-European Childhood Cancer Survivors: A PanCareSurFup and ProCardio Cohort and Nested Case-Control Study
Abstract
Purpose: Heart failure (HF) is a potentially life-threatening complication of treatment for childhood cancer. We evaluated the risk and risk factors for HF in a large European study of long-term survivors. Little is known of the effects of low doses of treatment, which is needed to improve current treatment protocols and surveillance guidelines.
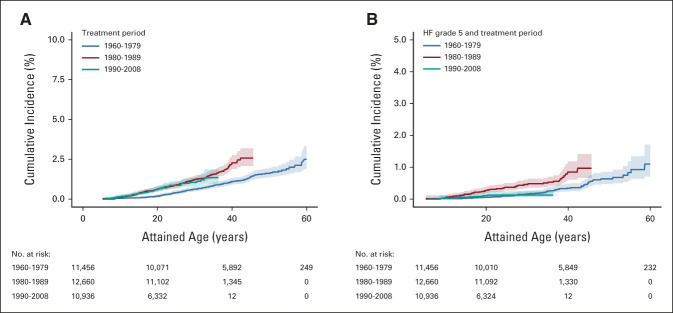
Methods: This study includes the PanCareSurFup and ProCardio cohort of ≥ 5-year childhood cancer survivors diagnosed between 1940 and 2009 in seven European countries (N = 42,361). We calculated the cumulative incidence of HF and conducted a nested case-control study to evaluate detailed treatment-related risk factors.
Results: The cumulative incidence of HF was 2% (95% CI, 1.7 to 2.2) by age 50 years. The case-control study (n = 1,000) showed that survivors who received a mean heart radiation therapy (RT) dose of 5 to < 15 Gy have an increased risk of HF (odds ratio, 5.5; 95% CI, 2.5 to 12.3), when compared with no heart RT. The risk associated with doses 5 to < 15 Gy increased with exposure of a larger heart volume. In addition, the HF risk increased in a linear fashion with higher mean heart RT doses. Regarding total cumulative anthracycline dose, survivors who received ≥ 100 mg/m2 had a substantially increased risk of HF and survivors treated with a lower dose showed no significantly increased risk of HF. The dose-response relationship appeared quadratic with higher anthracycline doses.
Conclusion: Survivors who received a mean heart RT dose of ≥ 5 Gy have an increased risk of HF. The risk associated with RT increases with larger volumes exposed. Survivors treated with < 100 mg/m2 total cumulative anthracycline dose have no significantly increased risk of HF. These new findings might have consequences for new treatment protocols for children with cancer and for cardiomyopathy surveillance guidelines.
Conflict of interest statement
No other potential conflicts of interest were reported.
Figures


References
-
- Gatta G, Botta L, Rossi S, et al. : Childhood cancer survival in Europe 1999-2007: Results of EUROCARE-5—A population-based study. Lancet Oncol 15:35-47, 2014 - PubMed
-
- van der Pal HJ, van Dalen EC, van Delden E, et al. : High risk of symptomatic cardiac events in childhood cancer survivors. J Clin Oncol 30:1429-1437, 2012 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
