

doi: 10.1080/10428194.2022.2118532.
Epub 2022 Sep 8.
A nomogram using cytogenetics, TP53, and NPM1 mutational status can predict responses to induction chemotherapy in AML
Affiliations
- PMID: 36075047
- PMCID: PMC9771947
- DOI: 10.1080/10428194.2022.2118532
Item in Clipboard
A nomogram using cytogenetics, TP53, and NPM1 mutational status can predict responses to induction chemotherapy in AML
Leuk Lymphoma.
2022 Dec.
No abstract available
Figures
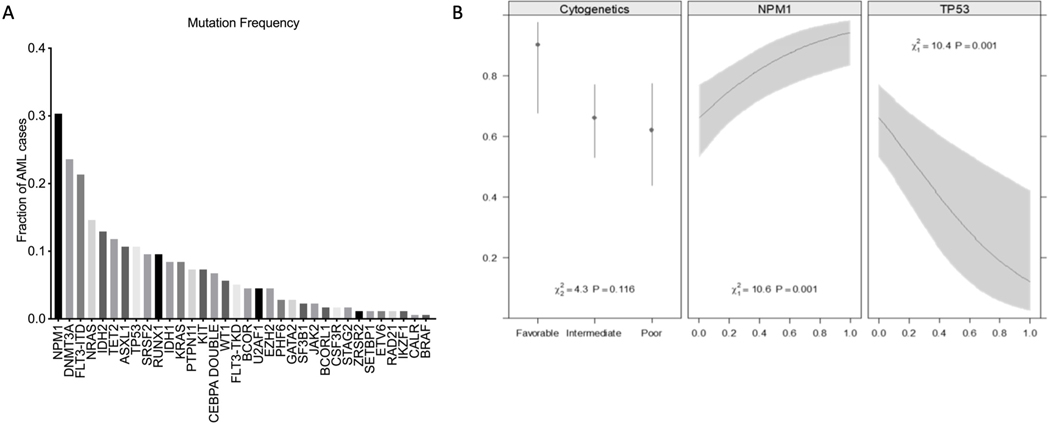
Among the genes, only NPM1, DNMT3A and TP53, were associated with response to intensive induction chemotherapy. B. Probability to response to induction chemotherapy. NPM1, TP53, and cytogenetic class were used to fit a multivariate logistic model for response to the first course of chemotherapy. The presence of a TP53 mutation and poor cytogenetics, and the absence of an NPM1 mutation have a low probability of response to induction chemotherapy. The model is summarized by the C index (area under the ROC curve) and R2 (proportion of variance explained). After bootstrap validation, these statistics were reduced to 0.781 and 0.319, respectively.
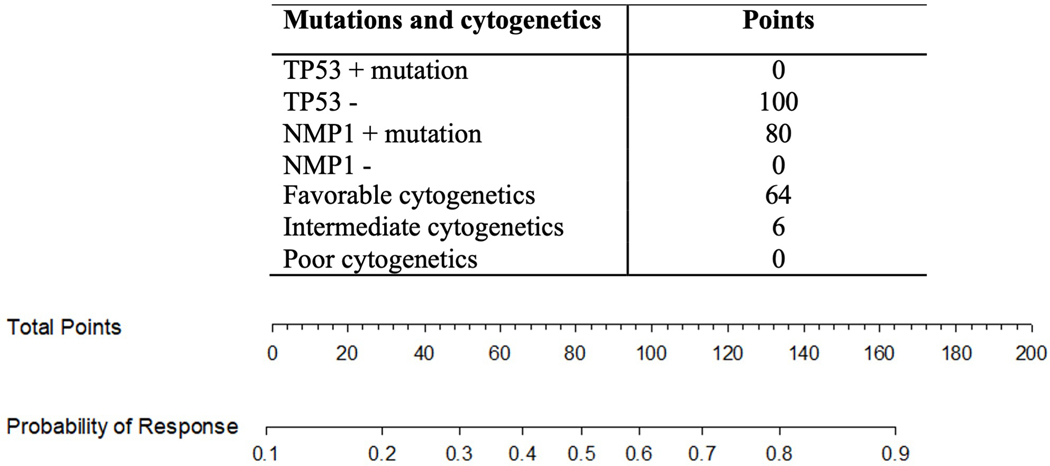
The nomogram is used to assign points to each of the 3 predictors (TP53, NPM1, cytogenetics). The combined points for an individual patient are then added and the total points are compared to the probability for response to induction chemotherapy. For example, a patient with NPM1 mutation, intermediate cytogenetics and no TP53 mutation has a combined 186 points and a >0.9 probability of response.
References
-
- Perl AE. The role of targeted therapy in the management of patients with AML. Blood Adv. 2017. Nov 14;1(24):2281–2294. doi: 10.1182/bloodadvances.2017009829. advisory committee for Asana Biosciences and Actinium Pharmaceuticals and has consulted for Daiichi Sankyo, Astellas, Novartis, Pfizer, Arog, Seattle Genetics, Asana Biosciences, and Actinium Pharmaceuticals. Off-label drug use: This presentation includes novel agents in clinical development that do not yet have label indications in acute myeloid leukemia (AML). The use of sorafenib, azacitidine, or decitabine for AML therapy is off label. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous