

Variations in Medicare Advantage Switching Rates Among African American and Hispanic Medicare Beneficiaries With Alzheimer's Disease and Related Dementias, by Sex and Dual Eligibility
- PMID: 36075080
- PMCID: PMC9923792
- DOI: 10.1093/geronb/gbac132
Variations in Medicare Advantage Switching Rates Among African American and Hispanic Medicare Beneficiaries With Alzheimer's Disease and Related Dementias, by Sex and Dual Eligibility
Abstract
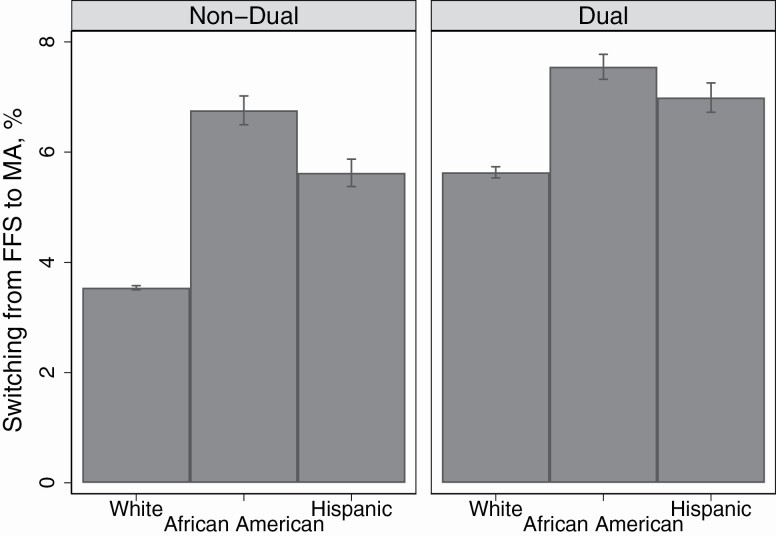
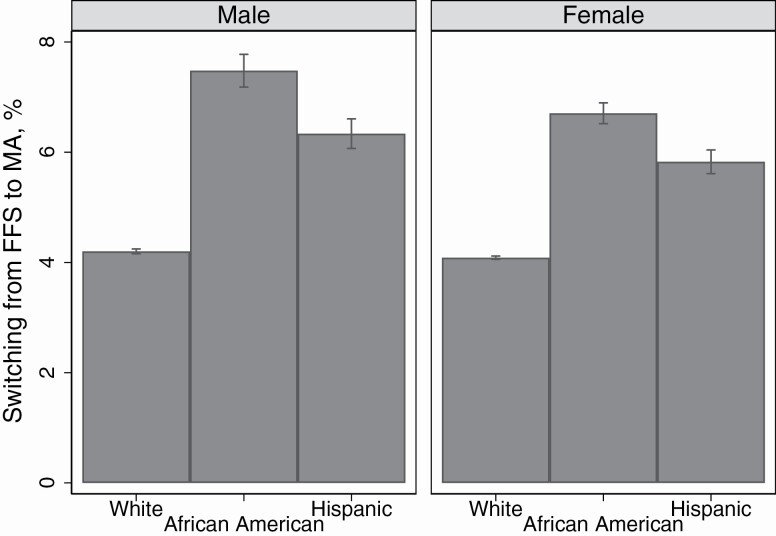
Objectives: The objective of this study was to identify rates of switching to Medicare Advantage (MA) among fee-for-service (FFS) Medicare beneficiaries with Alzheimer's disease and related dementias (ADRD) by race/ethnicity and whether these rates vary by sex and dual-eligibility status for Medicare and Medicaid.
Methods: Data came from the Medicare Master Beneficiary Summary File from 2017 to 2018. The outcome of interest for this study was switching from FFS to MA during any month in 2018. The primary independent variable was race/ethnicity including non-Hispanic White, non-Hispanic African American, and Hispanic beneficiaries. Two interaction terms among race/ethnicity and dual eligibility, and race/ethnicity and sex were included. The model adjusted for age, year of ADRD diagnosis, the number of chronic/disabling conditions, total health care costs, and ZIP code fixed effects.
Results: The study included 2,284,175 FFS Medicare beneficiaries with an ADRD diagnosis in 2017. Among dual-eligible beneficiaries, adjusted rates of switching were higher among African American (1.91 percentage points [p.p.], 95% confidence interval [CI]: 1.68-2.15) and Hispanic beneficiaries (1.36 p.p., 95% CI: 1.07-1.64) compared to non-Hispanic White beneficiaries. Among males, adjusted rates were higher among African American (3.28 p.p., 95% CI: 2.97-3.59) and Hispanic beneficiaries (2.14 p.p., 95% CI: 1.86-2.41) compared to non-Hispanic White beneficiaries.
Discussion: Among persons with ADRD, African American and Hispanic beneficiaries are more likely than White beneficiaries to switch from FFS to MA. This finding underscores the need to monitor the quality and equity of access and care for these populations.
Keywords: Dementia; Health care costs; Health insurance; Racial disparities.
© The Author(s) 2022. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
M. Rivera-Hernandez reported receiving grants form the National Institute on Aging during the conduct of the study. D. J. Meyers reported receiving grants from the National Institute on Aging and the National Institute on Minority Health and Health Disparities outside the submitted work. A. M. Trivedi reported receiving grants from the National Institute on Aging during the conduct of the study and receiving grants from the National Institute of Diabetes and Digestive and Kidney Diseases, the Agency for Healthcare Research and Quality and the Department of Veterans Affairs outside the submitted work.
Figures
References
-
- America’s Health Insurance Plans. (2019a). Medicare Advantage demographics report, 2016. https://www.ahip.org/wp-content/uploads/MA_Demographics_Report_2019.pdf
-
- America’s Health Insurance Plans. (2019b). State of Medigap 2019: Trends in enrollment and demographics. https://www.ahip.org/wp-content/uploads/IB_StateofMedigap2019.pdf
-
- Artiga, S. (2020, June 1). Health disparities are a symptom of broader social and economic inequities. KFF. https://www.kff.org/policy-watch/health-disparities-symptom-broader-soci...
-
- Boccuti, C., Jacobson, G., Orgera, K., & Newman, T. (2018, July 11). Medigap enrollment and consumer protections vary across states. KFF. https://www.kff.org/medicare/issue-brief/medigap-enrollment-and-consumer...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
