

Otopathologic and Computed Tomography Correlation of Internal Auditory Canal Diverticula in Otosclerosis
- PMID: 36075107
- PMCID: PMC9771591
- DOI: 10.1097/MAO.0000000000003665
Otopathologic and Computed Tomography Correlation of Internal Auditory Canal Diverticula in Otosclerosis
Abstract
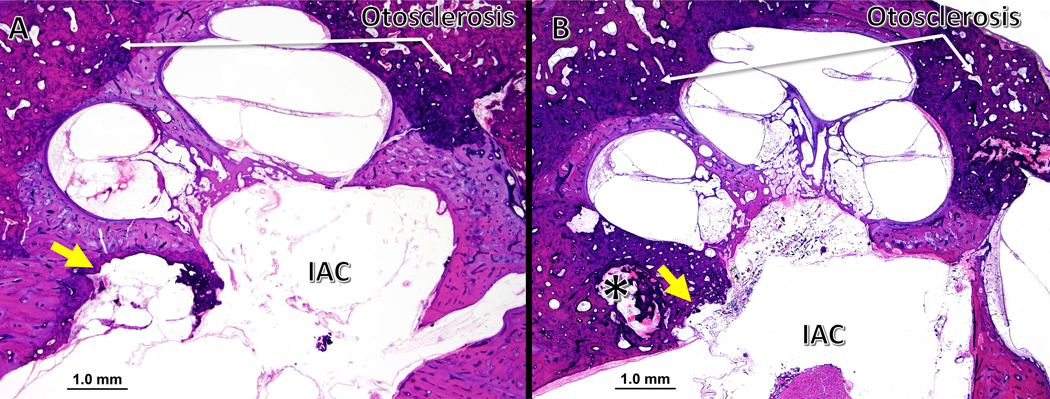
Introduction: Internal auditory canal (IAC) diverticula, also known as IAC cavitary lesions or anterior cupping of the IAC, observed in otopathologic specimens and high-resolution computed tomography (CT) scans of the temporal bone are thought to be related to otosclerosis. Herein, we examined the usefulness of CT scans in identifying diverticula and determined whether IAC diverticula are associated with otosclerosis on otopathology.
Methods: One hundred five consecutive specimens were identified from the National Temporal Bone Hearing and Balance Pathology Resource Registry. Inclusion criteria included the availability of histologic slides and postmortem specimen CT scans. Exclusion criteria included cases with severe postmortem changes or lesions causing bony destruction of the IAC.
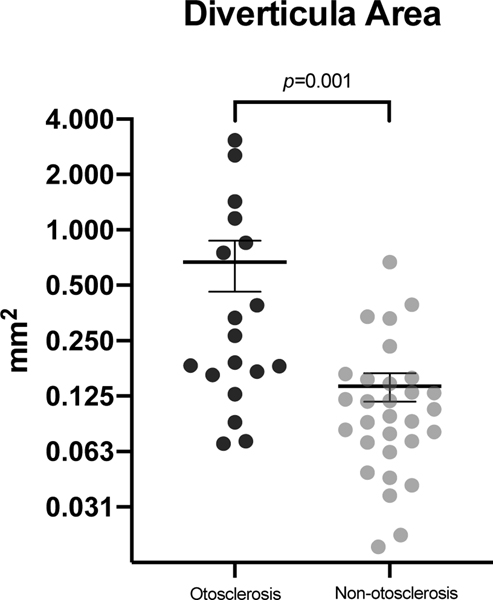
Results: Ninety-seven specimens met criteria for study. Of these, 42% of the specimens were from male patients, and the average age of death was 77 years (SD = 18 yr). IAC diverticula were found in 48 specimens, of which 46% were identified in the CT scans. The mean area of the IAC diverticula was 0.34 mm 2 . The sensitivity and specificity of detecting IAC diverticula based on CT were 77% and 63%, respectively. Overall, 27% of specimens had otosclerosis. Histologic IAC diverticula were more common in specimens with otosclerosis than those without (37.5% versus 16%; p = 0.019). Cases with otosclerosis had a greater mean histologic diverticula area compared with nonotosclerosis cases (0.69 mm 2 versus 0.14 mm 2 ; p = 0.001).
Conclusion: IAC diverticula are commonly found in otopathologic specimens with varied etiologies, but larger diverticula are more likely to be associated with otosclerosis. The sensitivity and specificity of CT scans to detect IAC diverticula are limited.
Copyright © 2022, Otology & Neurotology, Inc.
Conflict of interest statement
J.C. has a patent pending at Grace Medical. E.K. is a scientific advisor at Desktop Metal and has a patent pending at Grace Medical. H.S. is in the surgical advisory board of MedEl and a shareholder at Rescue Hearing. M.J.McK. is the co-founder and CMO of Akouos Inc. A.Q. has a sponsored research agreement with Frequency Therapeutics, sponsored research agreement, patent pending at Grace Medical, and consulting for Alcon. The remaining authors disclose no conflicts of interest.
Figures


References
-
- Schuknecht HF. Pathology of the ear. Philadelphia: Lea & Febiger, 1993.
-
- Quesnel A, McKenna M. Otosclerosis. In: Sataloff RT, Lalwani AK, eds. Sataloff’s Comprehensive Textbook of Otolaryngology: Head & Neck Surgery: Otology/Neurotology/Skull Base Surgery: JP Medical Ltd, 2015:231–242.
-
- Cureoglu S, Schachern PA, Ferlito A, Rinaldo A, Tsuprun V, Paparella MM. Otosclerosis: etiopathogenesis and histopathology. Am J Otolaryngol 2006; 27:334–340. - PubMed
-
- Karosi T, Sziklai I. Etiopathogenesis of otosclerosis. Eur Arch Otorhinolaryngol 2010; 267:1337–1349. - PubMed
-
- Roland P, Samy R. Otosclerosis. In: Bailey BJ, Johnson JT, Newlands SD, eds. Head & neck surgery--otolaryngology. Philadelphia, PA: Lippincott Williams & Wilkins, 2006:2126–2137.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
