

Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission
- PMID: 36075255
- PMCID: PMC11260396
- DOI: 10.1016/S0140-6736(22)01273-9
Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission
Abstract
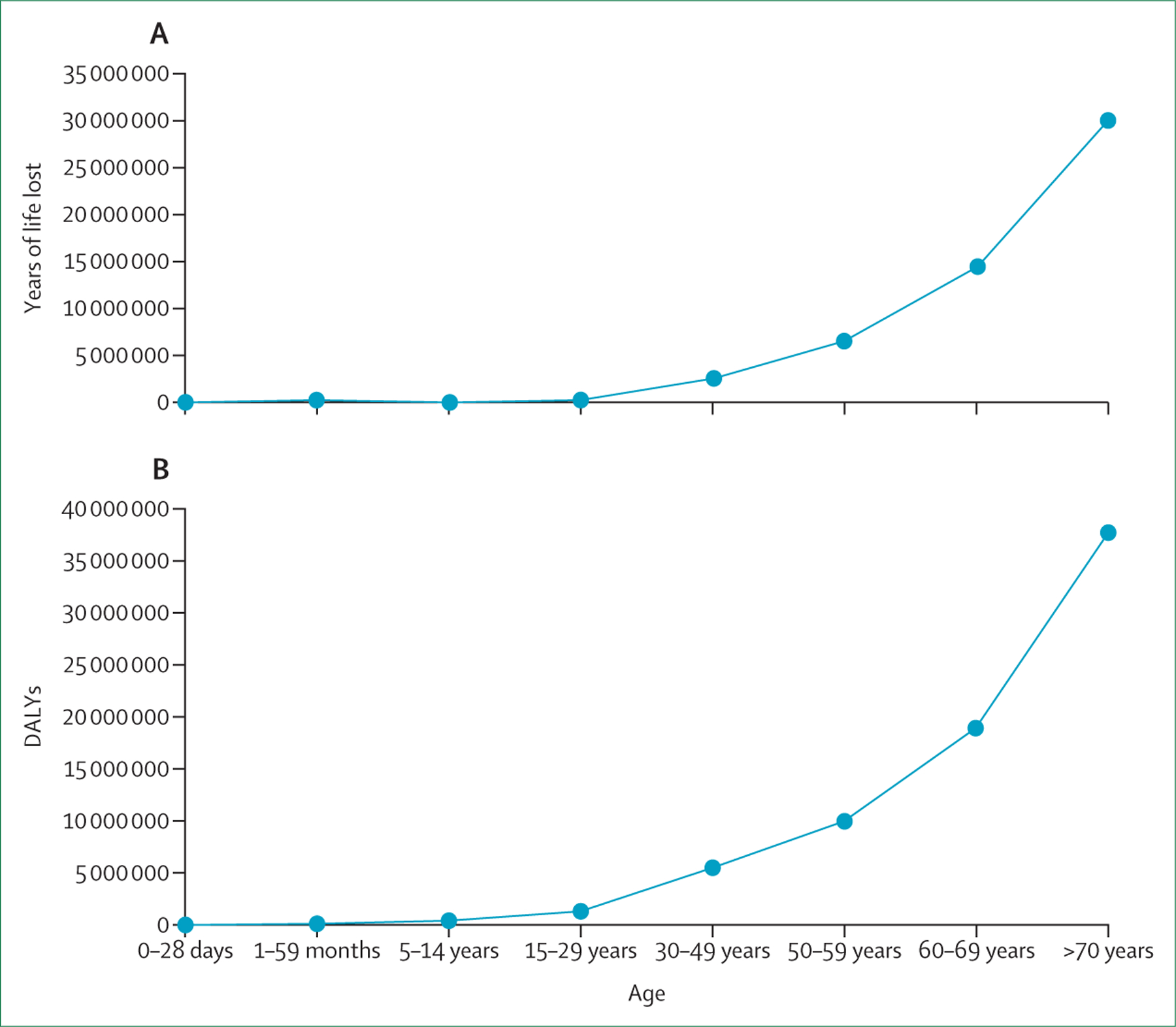
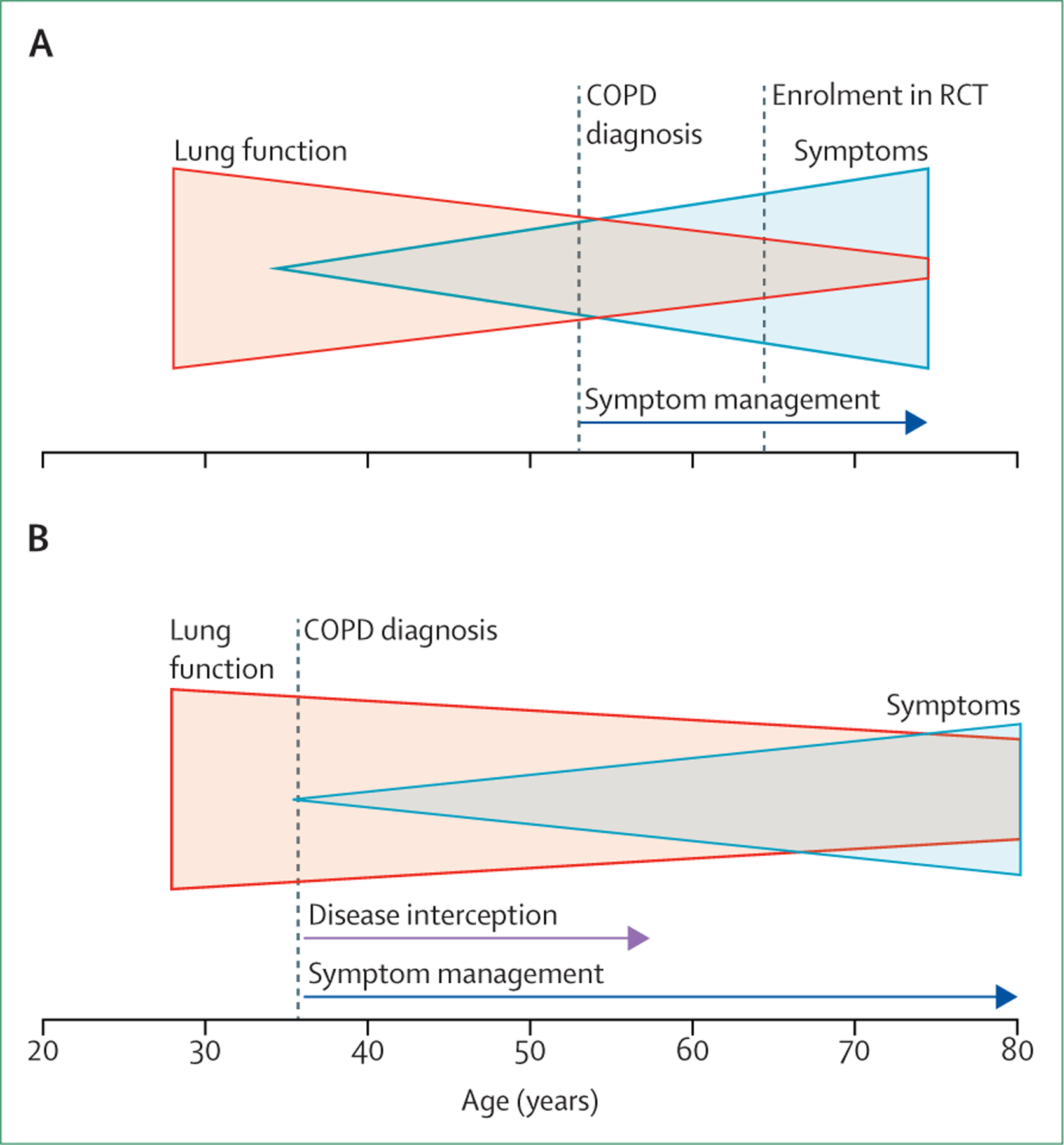
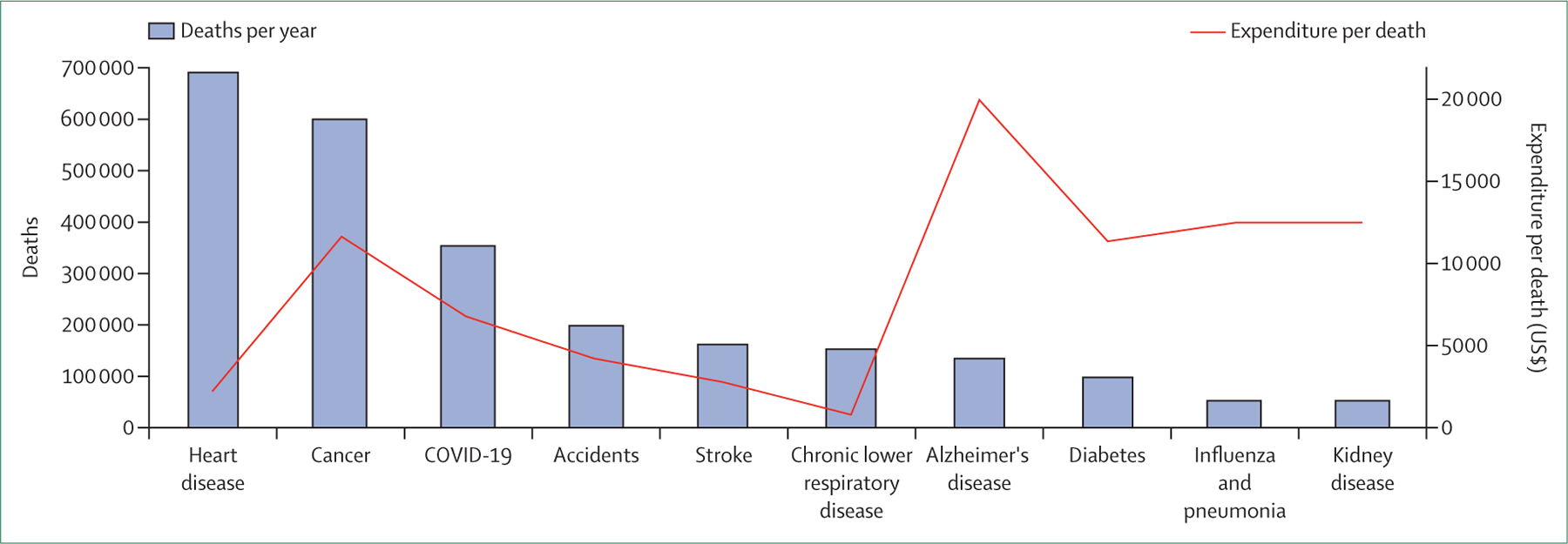
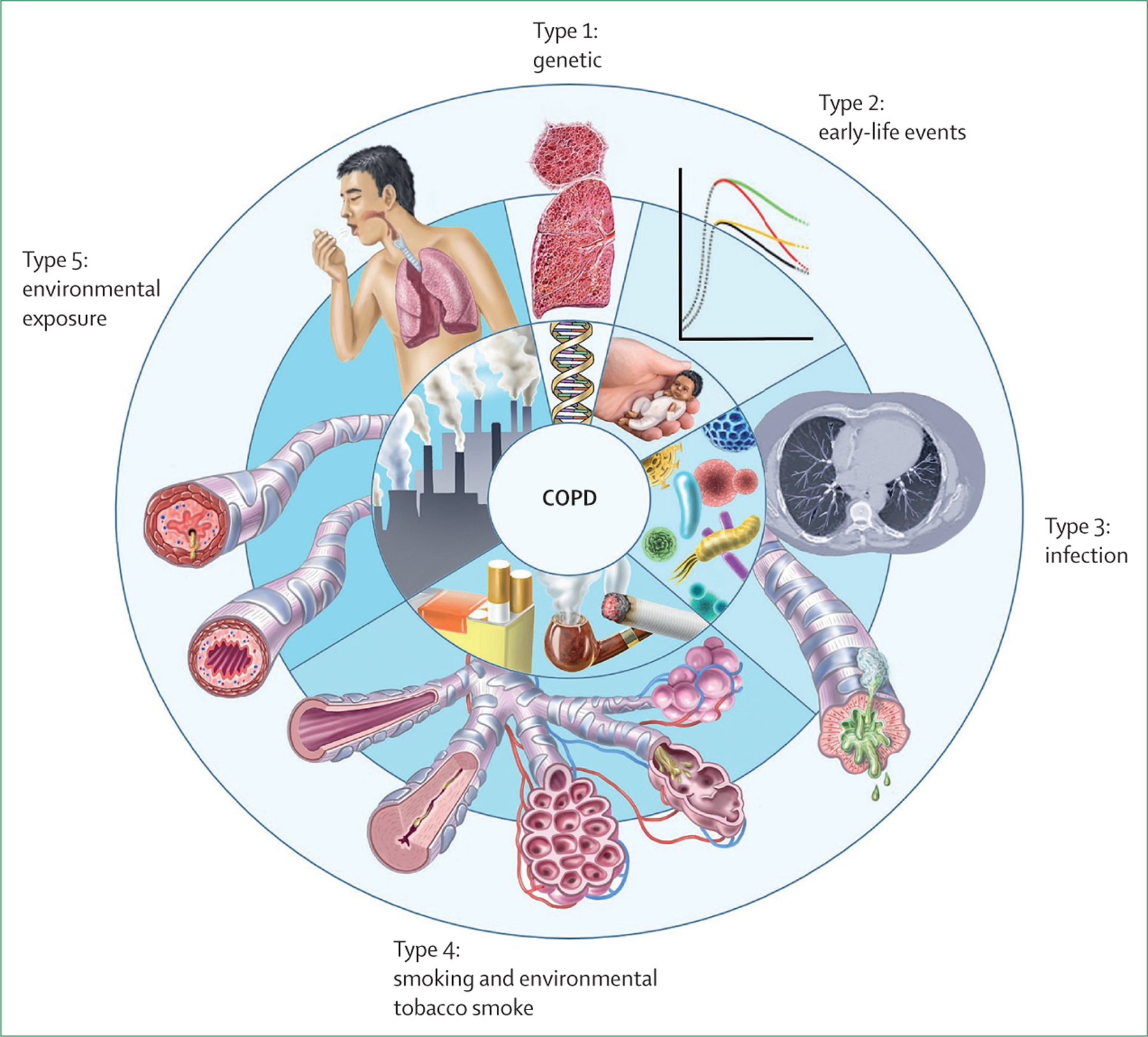
Despite substantial progress in reducing the global impact of many non-communicable diseases, including heart disease and cancer, morbidity and mortality due to chronic respiratory disease continues to increase. This increase is driven primarily by the growing burden of chronic obstructive pulmonary disease (COPD), and has occurred despite the identification of cigarette smoking as the major risk factor for the disease more than 50 years ago. Many factors have contributed to what must now be considered a public health emergency: failure to limit the sale and consumption of tobacco products, unchecked exposure to environmental pollutants across the life course, and the ageing of the global population (partly as a result of improved outcomes for other conditions). Additionally, despite the heterogeneity of COPD, diagnostic approaches have not changed in decades and rely almost exclusively on post-bronchodilator spirometry, which is insensitive for early pathological changes, underused, often misinterpreted, and not predictive of symptoms. Furthermore, guidelines recommend only simplistic disease classification strategies, resulting in the same therapeutic approach for patients with widely differing conditions that are almost certainly driven by variable pathophysiological mechanisms. And, compared with other diseases with similar or less morbidity and mortality, the investment of financial and intellectual resources from both the public and private sector to advance understanding of COPD, reduce exposure to known risks, and develop new therapeutics has been woefully inadequate.
Conflict of interest statement
Declaration of interests DS reports a grant from the Swiss National Foundation (SNF 320030_189280), and unrestricted grants from Curetis, AstraZeneca, and Boston Scientifics (paid to their institution); honoraria for participation in data safety monitoring or advisory boards or talks for CSL Behring, Berlin-Chemie Menarini, Novartis, GlaxoSmithKline, AstraZeneca, Vifor, Merck, Sanofi, Merck Sharp & Dohme, Boehringer Ingelheim, and Chiesi; and is the current Global Initiative for Chronic Obstructive Lung Disease (GOLD) representative for Switzerland, the immediate past Education Council Chair of the European Respiratory Society, and President of the Education Committee of the Swiss Respiratory Society. SYA reports grants from the US National Institutes of Health (K08HL145118) and the Pulmonary Fibrosis Foundation (the I M Rosenzweig Junior Investigator Award), and is an owner of Quantitative Imaging Solutions. AA reports unrestricted research grants from GlaxoSmithKline and AstraZeneca; consulting fees from GlaxoSmithKline, AstraZeneca, Sanofi and Merck Sharp & Dohme; and payment for lectures and presentations from GlaxoSmithKline, AstraZeneca, Chiesi, and Menarini. MH reports personal fees from GlaxoSmithKline, AstraZeneca, Boehringer Ingelheim, Cipla, Chiesi, Novartis, Pulmonx, Teva, Verona, Merck, Mylan, Sanofi, DevPro, Aerogen, Polarian, Regeneron, United Therapeutics, UpToDate, Altesa Biopharma, Medscape, NACE, and Integrity; has received either in-kind research support or funds paid to their institution from the US National Institutes of Health, Novartis, Sunovion, Nuvaira, Sanofi, AstraZeneca, Boehringer Ingelheim, Gala Therapeutics, Biodesix, the COPD Foundation, and the American Lung Association; has participated in data safety monitoring boards for Novartis and Medtronic (funds paid to their institution); and has received stock options from Meissa Vaccines and Altesa Biopharma. TMP reports an early career development grant (K23HL153672) from the US National Heart, Lung, and Blood Institute. MRvM's department received €2000 from the Clinic for Respiratory Medicine and Pulmonary Cell Research, University Hospital Basel (Basel, Switzerland) for calculating the smoking-attributable burden of COPD reported in the Commission. Her department also received an unrestricted grant of €198 000 from Boehringer Ingelheim to develop a health economic cost-effectiveness model of COPD. BS is supported by a National Institutes of Health grant (U01 HL-139466). JDC reports grants from or contracts with AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Gilead Sciences, Grifols, Insmed, and Novartis, and consulting fees from AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Janssen, Grifols, Zambon, Pfizer, Novartis, Chiesi, and Insmed. NMH reports grants from AstraZeneca, and payment or honoraria for presentations, speakers' bureaus, or participation on advisory boards from AstraZeneca, Novartis, and BI-Lilley. MTD reports grants or contracts from the American Lung Association, the US Department of Defense, and the US National Institutes of Health, consulting fees from AstraZeneca, GlaxoSmithKline, Novartis, Pulmonx, and Teva, and support for attending meetings from Pulmonx. YS has received support from the Science and Technology Commission of Shanghai Municipility (200Z2261200). TW has served as an advisory board member or received honoraria for lectures from AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Novartis, and has received research grants from the German Ministry for Research and Education, GlaxoSmithKline, and AstraZeneca. FMEF reports institutional study grants from AstraZeneca and personal fees for consultancy or presentations from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Merck Sharp & Dohme, and Novartis. SCD holds investigator-initiated grants from AstraZeneca and GlaxoSmithKline. DDS reports honoraria for speaking engagements for AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline. MB reports grants or contracts (to their institution) from AstraZeneca and Roche and consulting fees (paid to their institution) from AstraZeneca, Sanofi, and Roche; honoraria for lectures, presentations, speakers' bureaus, manuscript writing, or educational events from AstraZeneca, Sanofi, Chiesi, and GlaxoSmithKline; participation on an advisory board from AstraZeneca; and scientific advisor work for ProAxsis and Albushealth. NNH reports grants or contracts (to their institution) from the National Instiutes of Health, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and the COPD Foundation; and participation on data safety monitoring boards or advisory boards for AstraZeneca and GlaxoSmithKline. RK reports grants from the National Heart, Lung, and Blood Institute, the Respiratory Health Association, PneumRx, Spiration, and AstraZeneca, and personal fees from AstraZeneca, CVS Caremark, GlaxoSmithKline, CSA Medical, and Boehringer Ingelheim. GJC has received personal fees from Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Broncus Medical, Chiesi, CSA Medical, Eolo, Gala Therapeutics, GlaxoSmithKline, Helios Medical, Merck, Medtronic, Mereo BioPharma, NGM Biopharmaceuticals, Novartis, Nuvaira, Olympus, Philips, Pulmonx, Respironics, Respivant Sciences, the Implementation Group, Sanofi, Regeneron, Gilead, and Verona. GRW has been supported by the National Heart, Lung, and Blood Institute (grants R01 HL116473 and R01 HL122464). All other authors declare no competing interests.
Figures
Comment in
-
Mark Dransfield: breathing new ideas into COPD.Lancet. 2022 Sep 17;400(10356):879. doi: 10.1016/S0140-6736(22)01701-9. Epub 2022 Sep 5. Lancet. 2022. PMID: 36075253 No abstract available.
-
COPD: from an end-stage disease to lifelong lung health.Lancet. 2022 Sep 17;400(10356):863. doi: 10.1016/S0140-6736(22)01700-7. Epub 2022 Sep 5. Lancet. 2022. PMID: 36075254 No abstract available.
-
Classification of COPD: fostering prevention and precision medicine in the Lancet Commission on COPD.Lancet. 2022 Sep 17;400(10356):869-871. doi: 10.1016/S0140-6736(22)01660-9. Epub 2022 Sep 5. Lancet. 2022. PMID: 36075257 No abstract available.
-
The Lancet COPD Commission: broader questions remain.Lancet. 2023 May 13;401(10388):1568-1569. doi: 10.1016/S0140-6736(23)00555-X. Lancet. 2023. PMID: 37179112 No abstract available.
-
The Lancet COPD Commission: broader questions remain.Lancet. 2023 May 13;401(10388):1568. doi: 10.1016/S0140-6736(23)00553-6. Lancet. 2023. PMID: 37179113 No abstract available.
-
The Lancet COPD Commission: broader questions remain.Lancet. 2023 May 13;401(10388):1569-1570. doi: 10.1016/S0140-6736(23)00556-1. Lancet. 2023. PMID: 37179114 No abstract available.
References
-
- Polverino F, Celli B. The challenge of controlling the COPD epidemic: unmet needs. Am J Med 2018; 131: 1–6. - PubMed
-
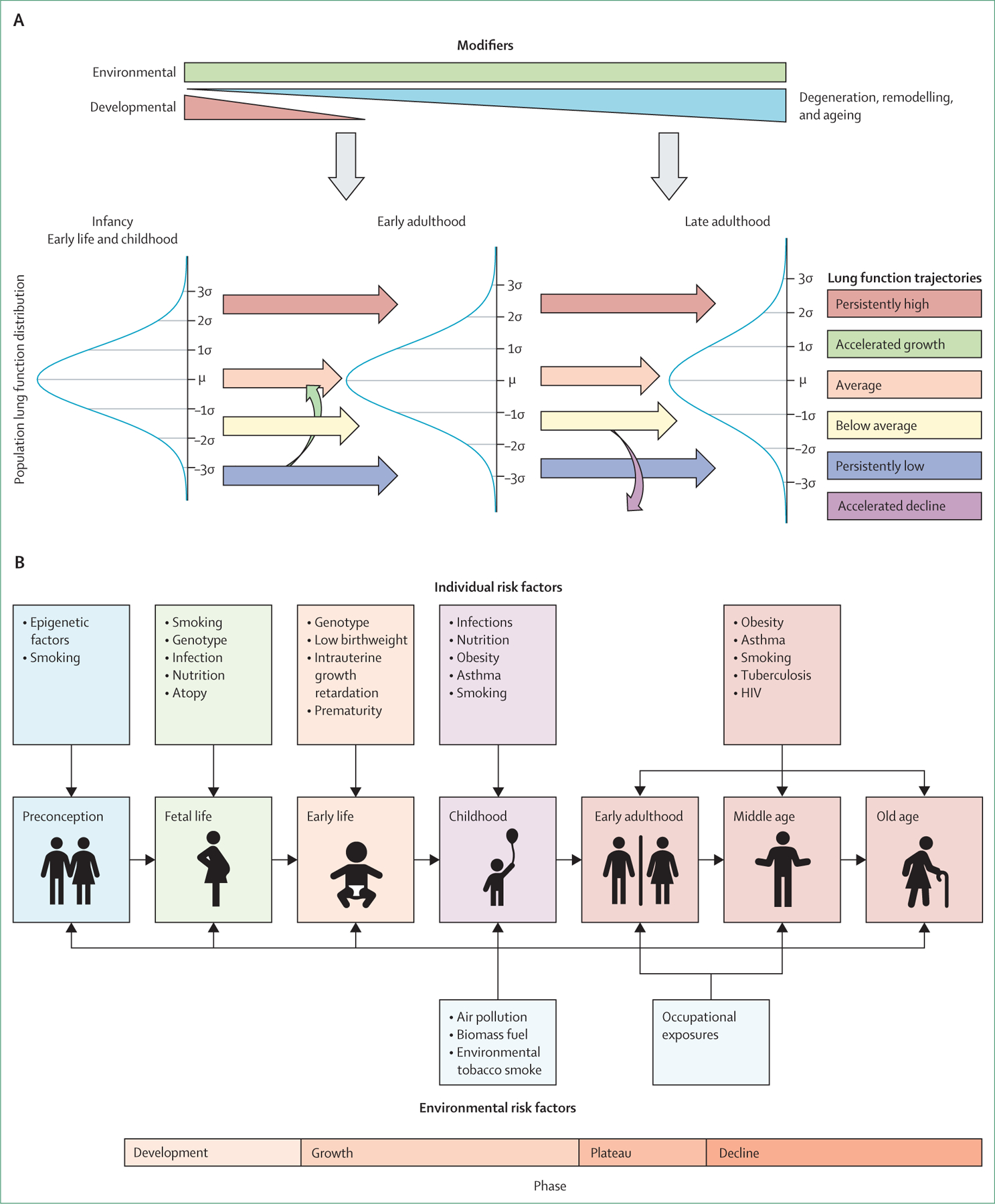
- Agustí A, Faner R. Lung function trajectories in health and disease. Lancet Respir Med 2019; 7: 358–64. - PubMed
-
- WHO Department of Data and Analytics. Global health estimates 2019: disease burden by cause, age, sex, by country and by region, 2000–2019. Geneva: World Health Organization, 2020.
-
- Singh D, Agusti A, Anzueto A, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J 2019; 53: 1900164. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
