

Gastrointestinal microbiota profile and clinical correlations in advanced EGFR-WT and EGFR-mutant non-small cell lung cancer
- PMID: 36076157
- PMCID: PMC9454126
- DOI: 10.1186/s12885-022-10050-3
Gastrointestinal microbiota profile and clinical correlations in advanced EGFR-WT and EGFR-mutant non-small cell lung cancer
Abstract
Introduction: Difference in clinical responses to cancer therapy in each patient is from several factors. Gastrointestinal microbiota is one of the reasons. However, this correlation remains unknown. This study aims to explore correlation between gastrointestinal microbiota profile and clinical outcomes in Thai advanced non-small cell lung cancer (NSCLC) according to epidermal growth factor receptor (EGFR) status.
Methods: We enrolled 13 patients with advanced EGFR-wild-type (WT) NSCLC who received chemotherapy and 15 patients with EGFR-mutant NSCLC who received EGFR tyrosine kinase inhibitors. We collected fecal samples at baseline and first disease evaluation and performed 16S rRNA gene sequencing by NGS to assess microbiota profile. The correlations between gastrointestinal microbiota and clinical variables were studied.
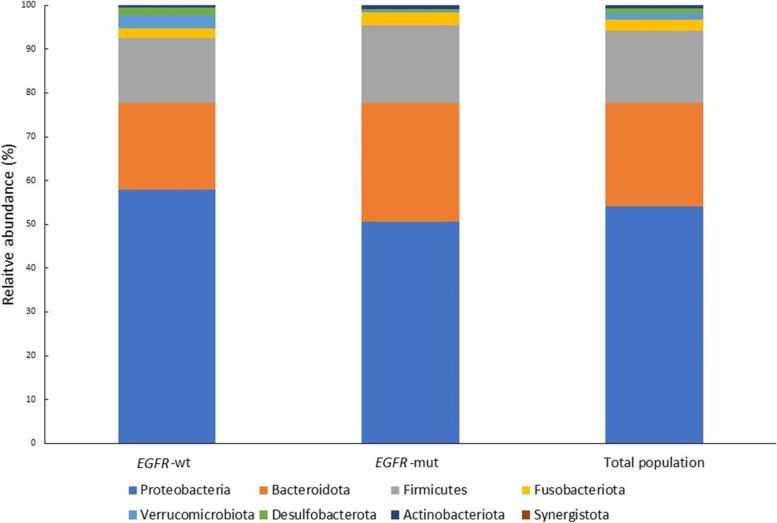
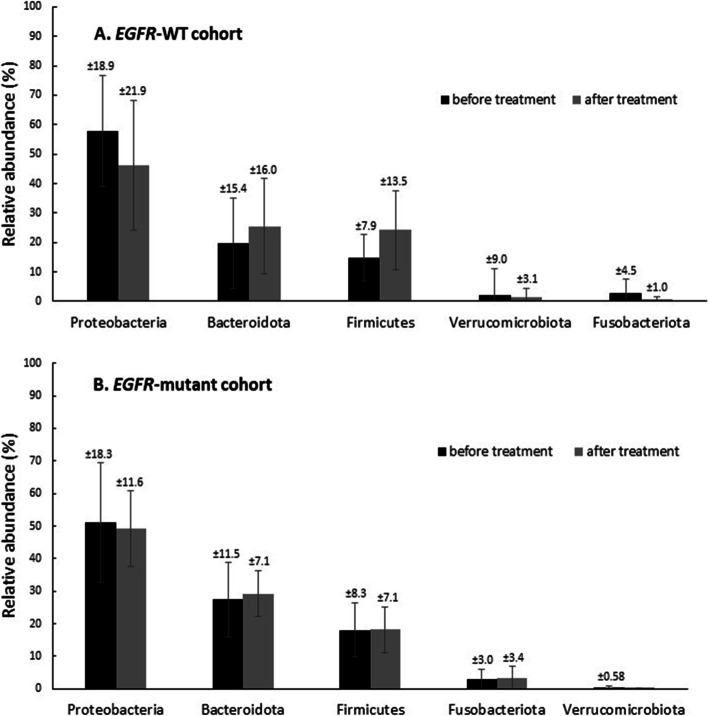
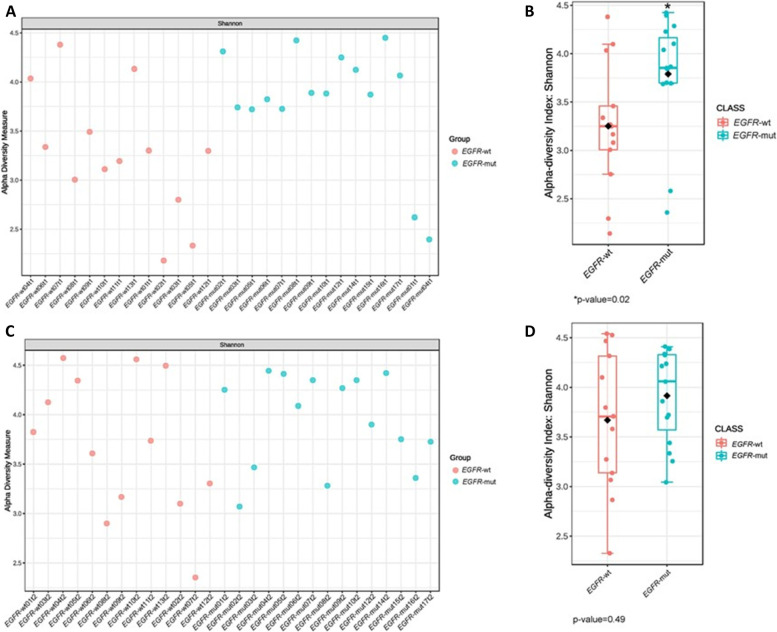
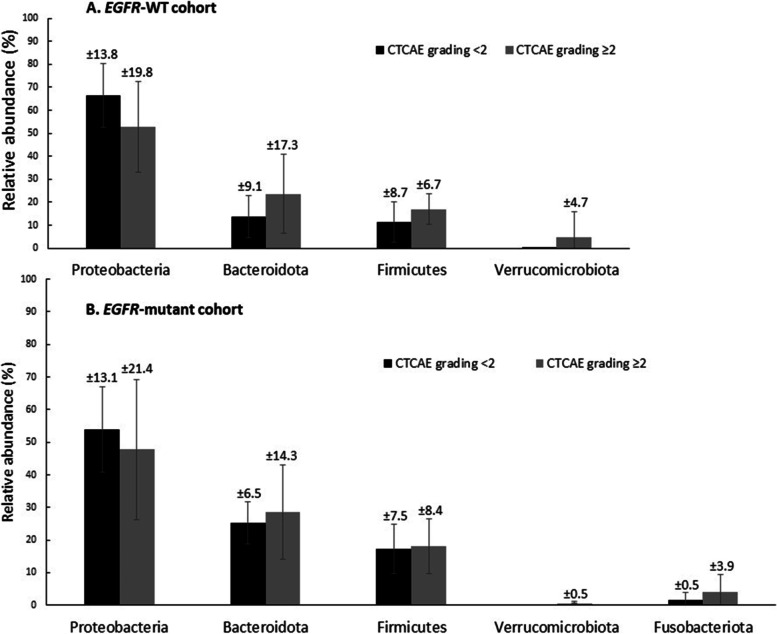
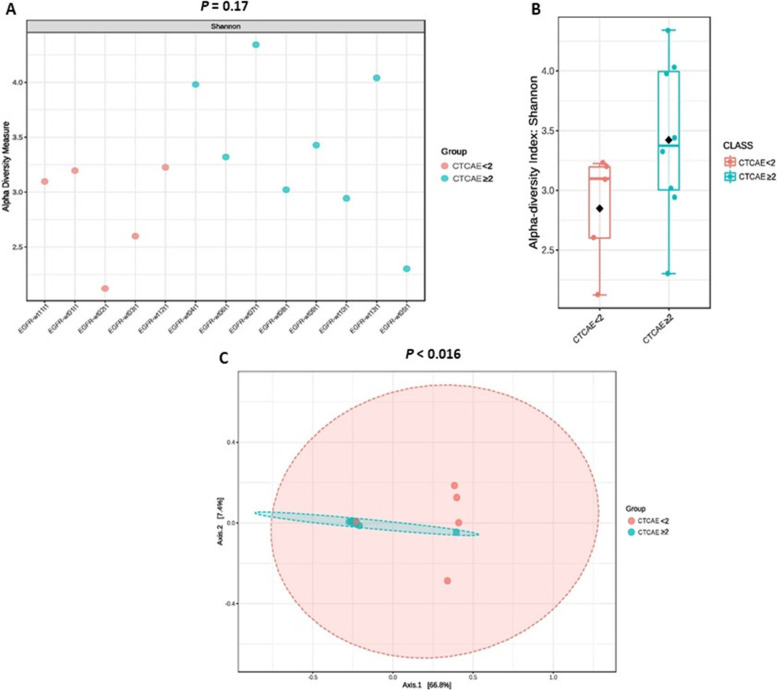
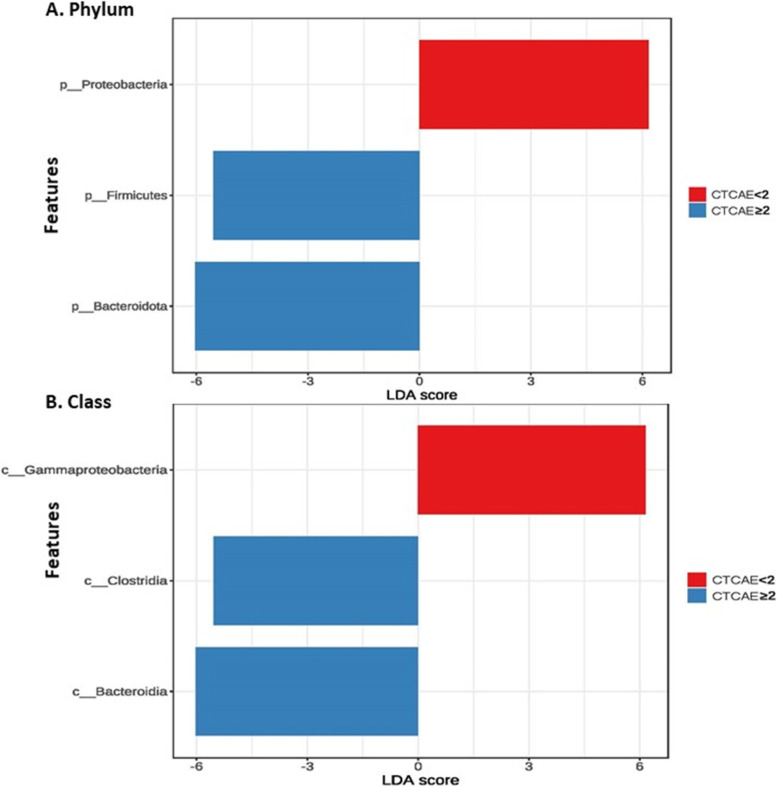
Results: The clinical characteristics were balanced between the cohorts, excluding significantly higher albumin levels in the EGFR-mutant group. Albumin was the only significant clinical factor affecting the treatment response in multivariate analysis (ORR 15.6%, P = 0.03). Proteobacteria counts were higher in the EGFR-WT group, whereas Bacteroidetes and Firmicutes counts were higher in the EGFR-mutant group. The alpha diversity of the gastrointestinal microbiome was significantly higher in the EGFR-mutant group (Shannon index: 3.82 vs. 3.25, P = 0.022). Following treatment, Proteobacteria counts were lower and Bacteroidetes and Firmicutes counts were higher in both cohorts; the changes were more prominent in the EGFR-WT cohort. No significant correlation between microbiota profile and treatment response were demonstrated in our study. However, beta diversity was significantly different according to severity of adverse events. Enrichment of Clostridia and Bacteroidia was associated with higher adverse event risk in the EGFR-WT cohort.
Conclusions: Proteobacteria was dominant in Thai lung cancer patients both EGFR-WT and EGFR-mutant, and this phylum maybe associate with lung cancer carcinogenesis. Chemotherapy altered the gastrointestinal microbiota, whereas EGFR-TKIs had less effects. Our findings highlight the potential predictive utility of the gastrointestinal microbiota for lung cancer carcinogenesis. Studies with larger cohorts and comparison with the healthy Thai population are ongoing to validate this pilot study.
Keywords: EGFR-mutant; Lung cancer; Microbiome; Microbiota; NSCLC.
© 2022. The Author(s).
Conflict of interest statement
All authors declare no competing interests to this study.
Figures
References
-
- Society TAC. Key Statistics for Lung Cancer 2020. https://www.cancer.org/cancer/lung-cancer/about/key-statistics.html.
-
- National Comprehensive Cancer Network. Non-small cell lung cancer (version 4.2021). https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed 3 Mar 2021.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
