

Takostubo syndrome combined with ventricular septal perforation: a case report
- PMID: 36076178
- PMCID: PMC9461131
- DOI: 10.1186/s12872-022-02834-z
Takostubo syndrome combined with ventricular septal perforation: a case report
Abstract
Background: The precise clinical features and etiologic basis of Takotsubo syndrome remain unclear, although an association with emotional or stressful triggers has been recognized. Ventricular septal perforation is a very rare life-threatening complication.
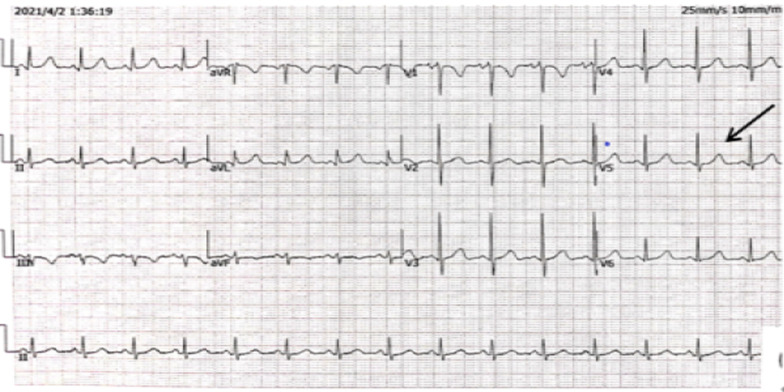
Case presentation: A 77-year-old female patient presented to the hospital with unrelieved chest tightness and shortness of breath. Three months ago, the patient's electrocardiogram revealed ischemic T wave inversion of the anterior wall, along with an increase in myocardial injury markers. There was no evidence of a ventricular septal defect on echocardiography. The patient was admitted to the respiratory department to treat lung lesions. The electrocardiogram demonstrated dynamic changes following admission, and the myocardial markers returned to normal, but the echocardiography revealed a ventricular septal defect. The initial diagnosis was ventricular septal perforation because of myocardial infarction with acute anterior ST-segment elevation. Coronary angiography revealed no abnormalities, but left ventricular angiography revealed an enlarged apex and VSD, with a right ventricular shunt bundle. Later, cardiac MRI revealed an apical ventricular septal defect. Further inquiry of the patient's medical history revealed that her husband died unexpectedly three months ago, and her daughter was seriously injured in a car accident, causing the patient severe emotional distress. Takotsubo syndrome was then determined in conjunction with the patient's medical history, symptoms, signs, and pertinent examinations. Without using a catheter or a surgical procedure, we managed the patient's medical condition. Two weeks later, the patient was discharged with symptoms improved.
Conclusions: Takotsubo syndrome is comparable to an acute myocardial infarction on clinical and electrocardiographic examination in the absence of significant coronary disease. Although ventricular septal perforation is most commonly associated with acute myocardial infarction, it can also happen following Takotsubo syndrome. Takotsubo syndrome complicated by ventricular septal perforation is easily misdiagnosed. The early recognition and management of this condition can avoid or reduce morbidity and mortality.
Keywords: Case report; Takotsubo syndrome; Ventricular septal perforation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
