

Determining the Potential of DNA Damage Response (DDR) Inhibitors in Cervical Cancer Therapy
- PMID: 36077823
- PMCID: PMC9454916
- DOI: 10.3390/cancers14174288
Determining the Potential of DNA Damage Response (DDR) Inhibitors in Cervical Cancer Therapy
Abstract
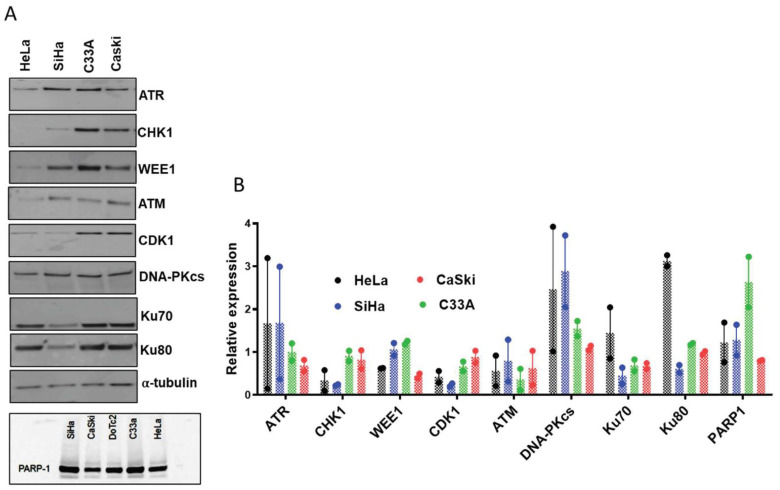
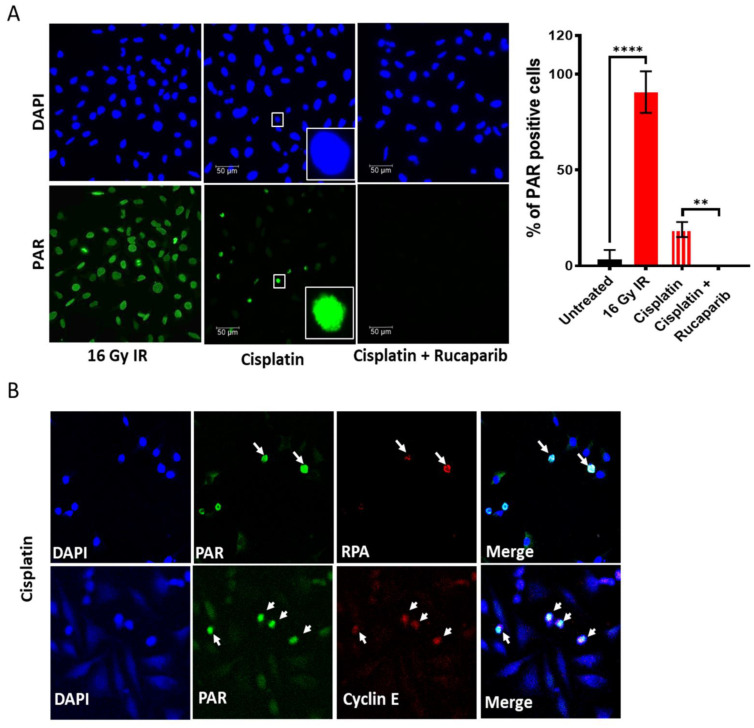
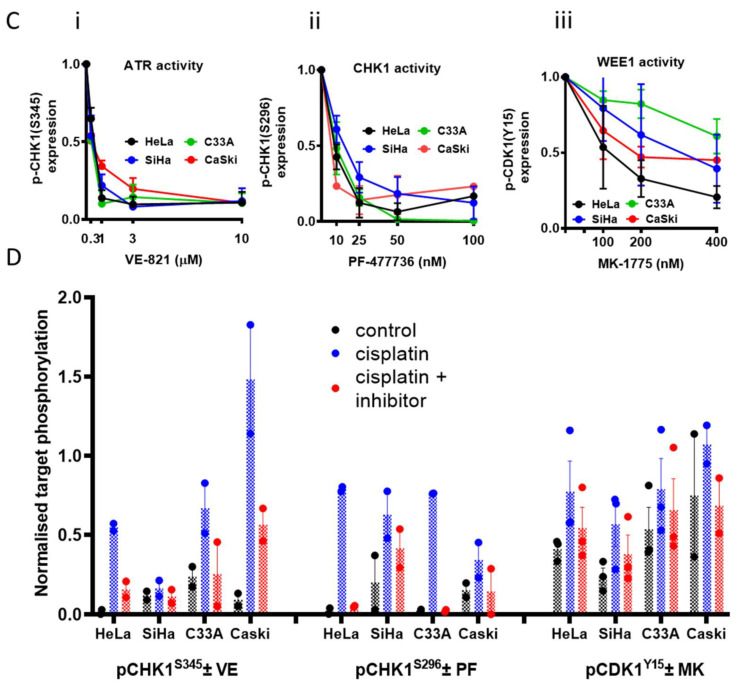
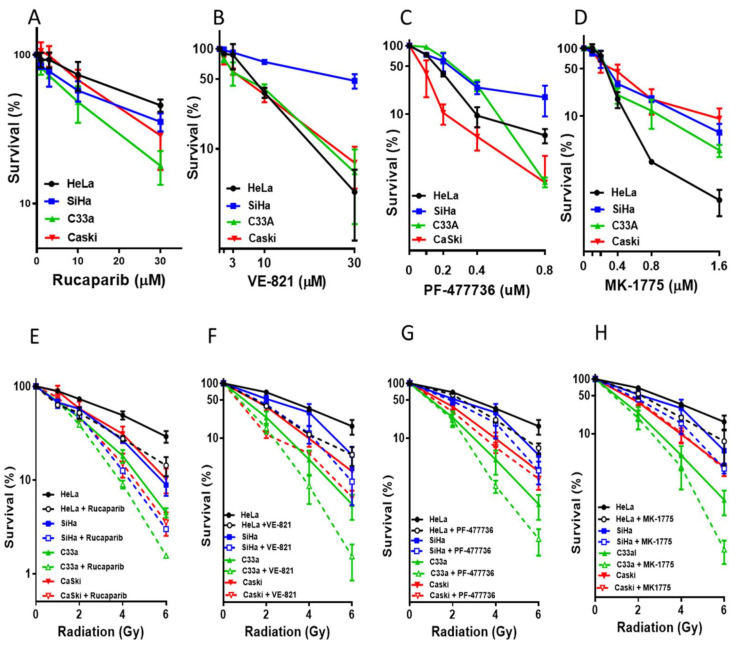
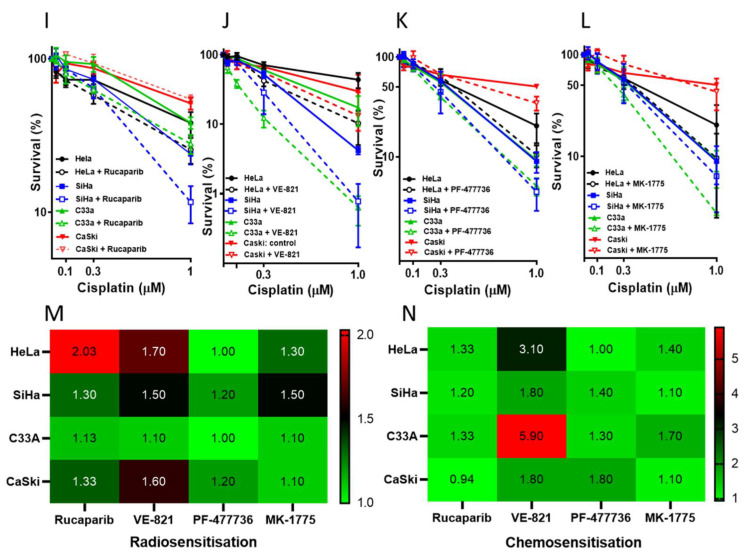
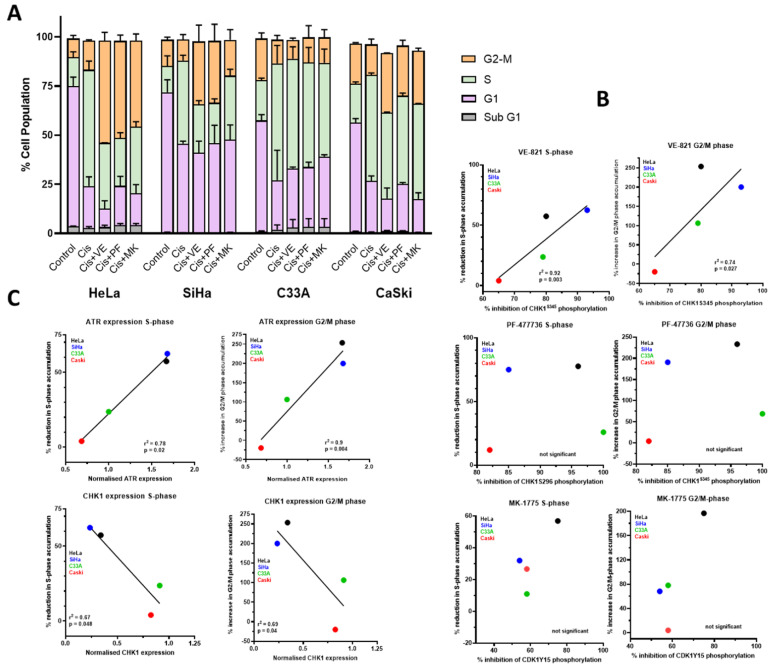
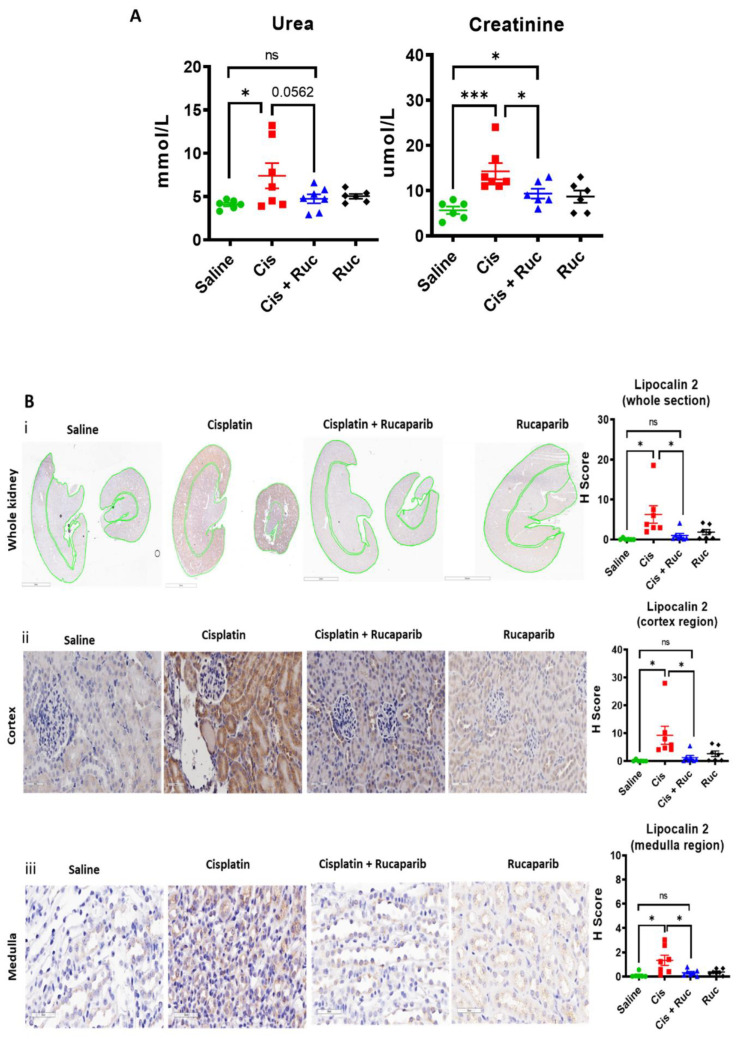
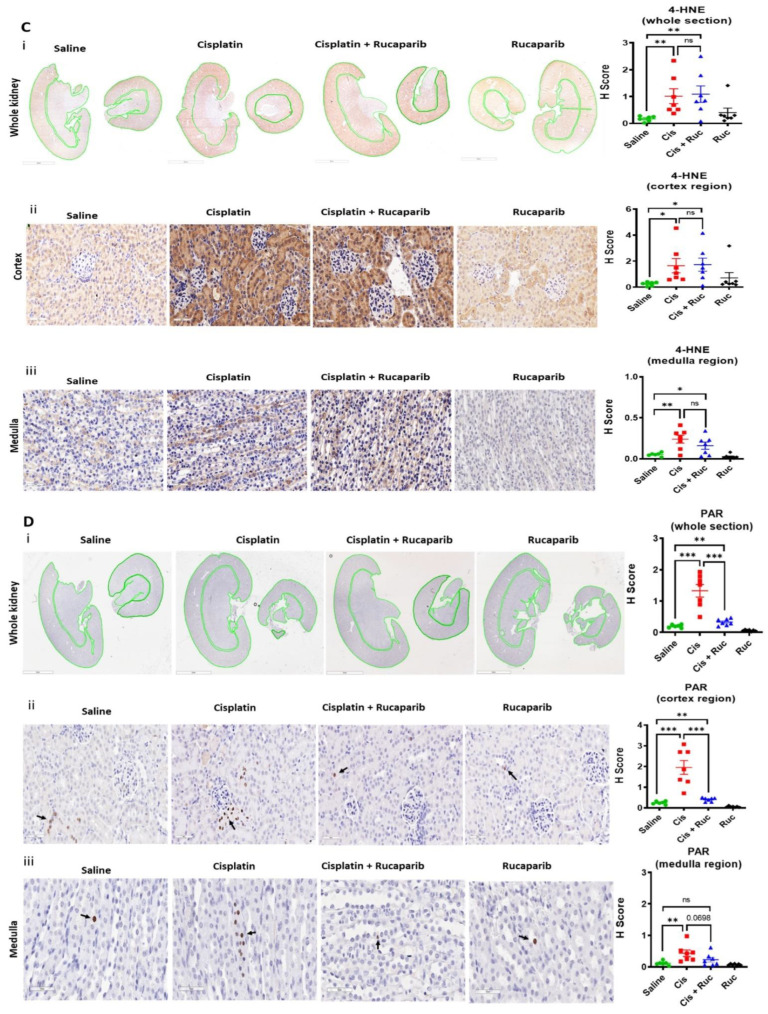
Cisplatin-based chemo-radiotherapy (CRT) is the standard treatment for advanced cervical cancer (CC) but the response rate is poor (46-72%) and cisplatin is nephrotoxic. Therefore, better treatment of CC is urgently needed. We have directly compared, for the first time, the cytotoxicity of four DDR inhibitors (rucaparib/PARPi, VE-821/ATRi, PF-477736/CHK1i and MK-1775/WEE1i) as single agents, and in combination with cisplatin and radiotherapy (RT) in a panel of CC cells. All inhibitors alone caused concentration-dependent cytotoxicity. Low ATM and DNA-PKcs levels were associated with greater VE-821 cytotoxicity. Cisplatin induced ATR, CHK1 and WEE1 activity in all of the cell lines. Cisplatin only activated PARP in S-phase cells, but RT activated PARP in the entire population. Rucaparib was the most potent radiosensitiser and VE-821 was the most potent chemosensitiser. VE-821, PF-47736 and MK-1775 attenuated cisplatin-induced S-phase arrest but tended to increase G2 phase accumulation. In mice, cisplatin-induced acute kidney injury was associated with oxidative stress and PARP activation and was prevented by rucaparib. Therefore, while all inhibitors investigated may increase the efficacy of CRT, the greatest clinical potential of rucaparib may be in limiting kidney damage, which is dose-limiting.
Keywords: DDR inhibitors; cervical cancer; cisplatin; kidney toxicity; radiotherapy.
Conflict of interest statement
N.C. was involved in the development of rucaparib and has received research funding for this work in the past and from Vertex and Merck for studies on VE-821. K.J.M. has received consultancy income from Bath ASU, Freeline Therapeutics & MPM Capital as well as grant income from Gemini Therapeutics & Catalyst Biosciences. A.M. received Royalty from Newcastle University for contributing to the development of rucaparib.
Figures
References
-
- Cervical Cancer Statistics. [(accessed on 25 July 2022)]. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/s....
-
- Boussios S., Seraj E., Zarkavelis G., Petrakis D., Kollas A., Kafantari A., Assi A., Tatsi K., Pavlidis N., Pentheroudakis G. Management of patients with recurrent/advanced cervical cancer beyond first line platinum regimens: Where do we stand? A literature review. Crit. Rev. Oncol. 2016;108:164–174. doi: 10.1016/j.critrevonc.2016.11.006. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
