

Prevalence, Characteristics, Management and Outcomes of Patients with Heart Failure with Preserved, Mildly Reduced, and Reduced Ejection Fraction in Spain
- PMID: 36079133
- PMCID: PMC9456780
- DOI: 10.3390/jcm11175199
Prevalence, Characteristics, Management and Outcomes of Patients with Heart Failure with Preserved, Mildly Reduced, and Reduced Ejection Fraction in Spain
Abstract
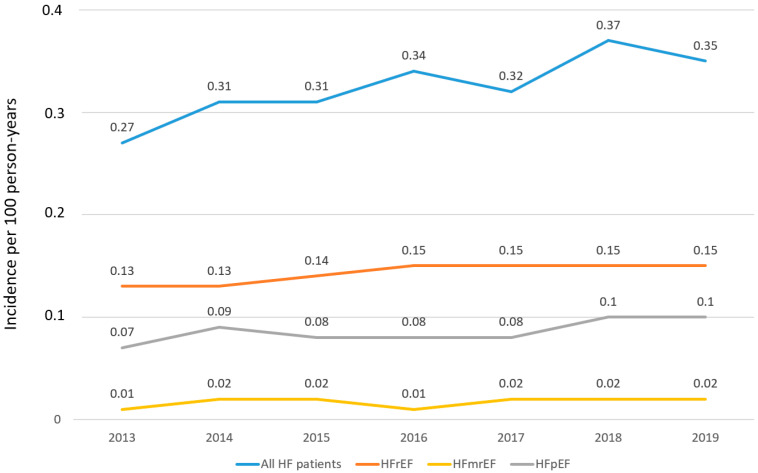
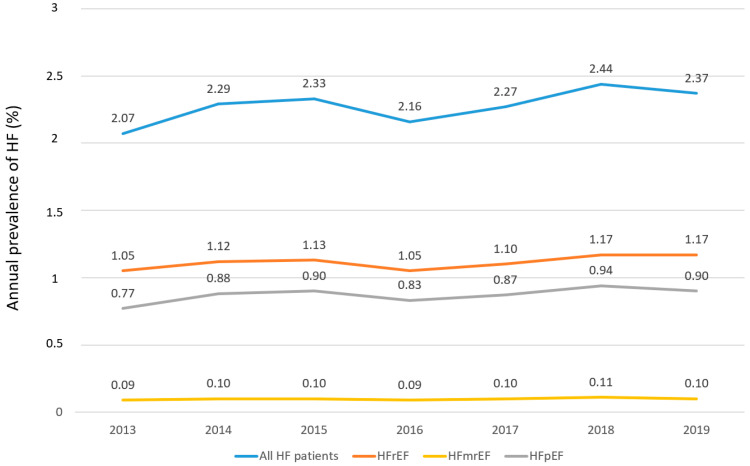
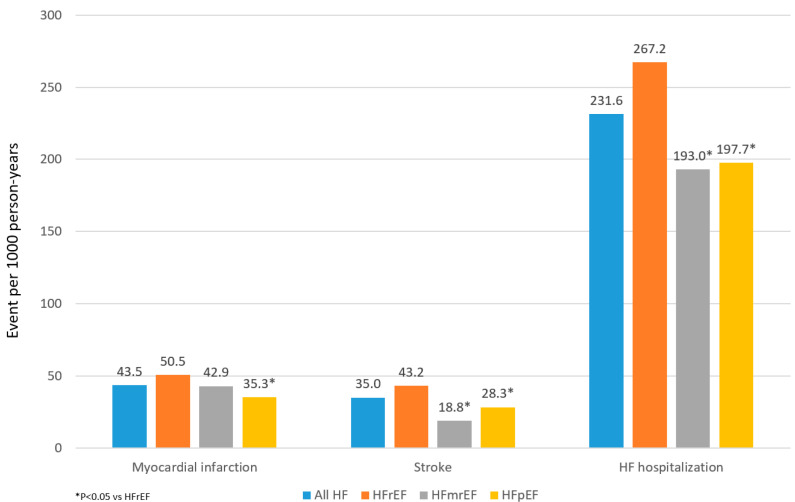
Objective: To estimate the prevalence, incidence, and describe the characteristics and management of patients with heart failure with preserved (HFpEF), mildly reduced (HFmrEF), and reduced ejection fraction (HFrEF) in Spain. Methods: Adults with ≥1 inpatient or outpatient HF diagnosis between 1 January 2013 and 30 September 2019 were identified through the BIG-PAC database. Annual incidence and prevalence by EF phenotype were estimated. Characteristics by EF phenotype were described in the 2016 and 2019 HF prevalent cohorts and outcomes in the 2016 HF prevalent cohort. Results: Overall, HF incidence and prevalence were 0.32/100 person-years and 2.34%, respectively, but increased every year. In 2019, 49.3% had HFrEF, 38.1% had HFpEF, and 4.3% had HFmrEF (in 8.3%, EF was not available). Compared with HFrEF, patients with HFpEF were largely female, older, and had more atrial fibrillation but less atherosclerotic cardiovascular disease. Among patients with HFrEF, 76.3% were taking renin-angiotensin system inhibitors, 69.5% beta-blockers, 36.8% aldosterone antagonists, 12.5% sacubitril/valsartan and 6.7% SGLT2 inhibitors. Patients with HFpEF and HFmrEF took fewer HF drugs compared to HFrEF. Overall, the event rates of HF hospitalization were 231.6/1000 person-years, which is more common in HFrEF patients. No clinically relevant differences were found in patients with HFpEF, regardless EF (50- < 60% vs. ≥60%). Conclusions: >2% of patients have HF, of which around 50% have HFrEF and 40% have HFpEF. The prevalence of HF is increasing over time. Clinical characteristics by EF phenotype are consistent with previous studies. The risk of outcomes, particularly HF hospitalization, remains high, likely related to insufficient HF treatment.
Keywords: SGLT2 inhibitors; cardiovascular; heart failure; sacubitril/valsartan.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., Alonso A., Beaton. A.Z., Bittencourt M.S., Boehme A.K., Buxton A.E., Carson A.P., Commodore-Mensah Y., et al. Heart Disease and Stroke Statistics-2022 Update: A Report From the American Heart Association. Circulation. 2022;145:e153–e639. doi: 10.1161/CIR.0000000000001052. - DOI - PubMed
-
- Cordero A., Rodríguez-Mañero M., Bertomeu-González V., García-Acuña J.M., Baluja A., Agra-Bermejo R., Álvarez-Álvarez B., Cid B., Zuazola P., González-Juanatey J.R. New-onset heart failure after acute coronary syndrome in patients without heart failure or left ventricular dysfunction. Rev. Esp. Cardiol. 2021;74:494–501. doi: 10.1016/j.recesp.2020.03.020. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
