

Association of Gut Microbiota with Atherogenic Dyslipidemia, and Its Impact on Serum Lipid Levels after Bariatric Surgery
- PMID: 36079803
- PMCID: PMC9460232
- DOI: 10.3390/nu14173545
Association of Gut Microbiota with Atherogenic Dyslipidemia, and Its Impact on Serum Lipid Levels after Bariatric Surgery
Abstract
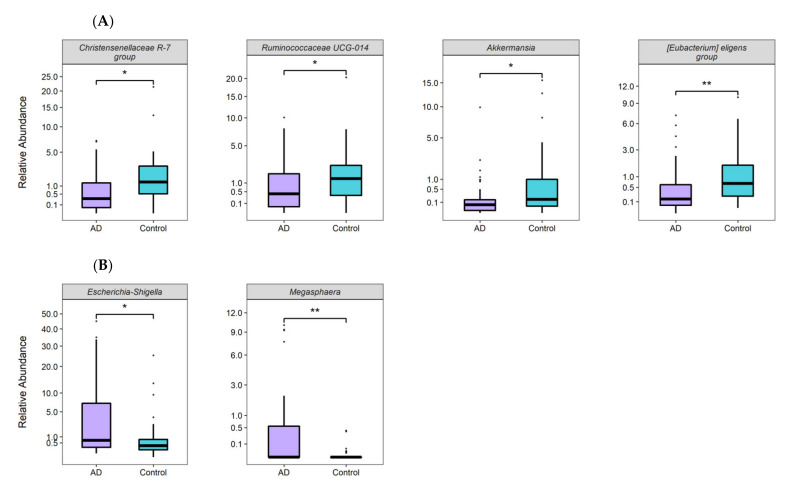
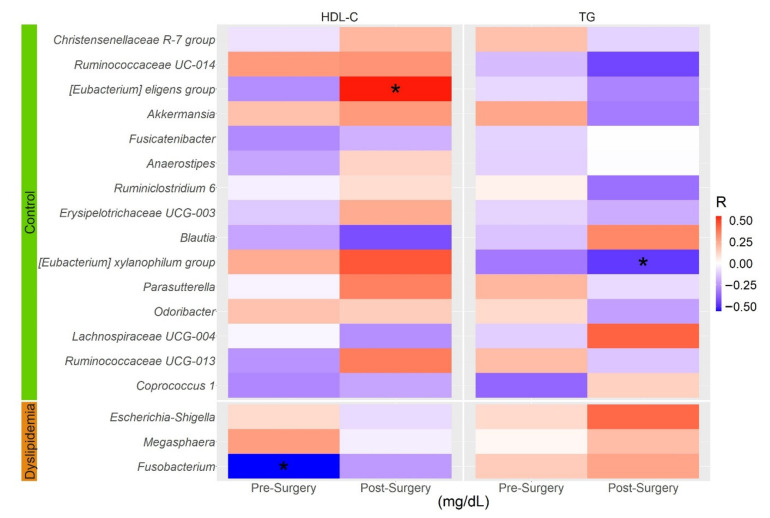
Gut microbiota has been suggested to modulate circulating lipids. However, the relationship between the gut microbiota and atherogenic dyslipidemia (AD), defined as the presence of both low HDL-C and hypertriglyceridemia, is not fully understood. Moreover, because obesity is among the main causes of secondary AD, it is important to analyze the effect of gut microbiota composition on lipid profiles after a weight loss intervention. We compared the microbial diversity and taxonomic composition in patients with AD (n = 41) and controls (n = 38) and sought correlations of genera abundance with serum lipid levels in 20 patients after weight loss induced by Roux-en-Y gastric bypass (RYGB) surgery. Gut microbiota composition was profiled using next-generation sequencing of 16S rRNA. Gut microbiota diversity was significantly lower in atherogenic dyslipidemia. Moreover, relative abundance of two genera with LDA score >3.5 (Megasphaera and LPS-producing Escherichia-Shigella), was significantly higher in AD subjects, while the abundance of four short chain fatty acids (SCFA) producing-genera (Christensenellaceae R-7, Ruminococcaceae UCG-014; Akkermansia and [Eubacterium] eligens group) was significantly higher in controls. Notably, [Eubacterium] eligens group abundance was also significantly associated with higher HDL-C levels in RYGB patients one year after surgery. Although dietary polyunsaturated fatty acid/saturated fatty acid (PUFA/SFA) ratio and PUFA intake were higher in controls than in AD subjects, of the four genera differentiated in cases and controls, only Akkermansia abundance showed a positive and significant correlation with PUFA/SFA ratio. Our results suggest that SCFA-producing bacteria promote a healthy lipid homeostasis, while the presence of LPS-producing bacteria such Escherichia-Shigella may contribute to the development of atherogenic dyslipidemia.
Keywords: 16S rRNA; HDL-C; dyslipidemia; gut microbiota; triglycerides.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures






References
-
- Carroll M., Kit B., Lacher D. Trends in elevated triglyceride in adults: United States, 2001–2012. NCHS Data Brief. 2015;198:198. - PubMed
-
- Aguilar-Salinas C.A., Olaiz G., Valles V., Torres J.M., Gómez Pérez F.J., Rull J.A., Rojas R., Franco A., Sepulveda J. High prevalence of low HDL cholesterol concentrations and mixed hyperlipidemia in a Mexican nationwide survey. J. Lipid Res. 2001;42:1298–1307. doi: 10.1016/S0022-2275(20)31581-9. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
