

Analysis of immune status in gastric adenocarcinoma with different infiltrating patterns and origin sites
- PMID: 36081505
- PMCID: PMC9445833
- DOI: 10.3389/fimmu.2022.978715
Analysis of immune status in gastric adenocarcinoma with different infiltrating patterns and origin sites
Abstract
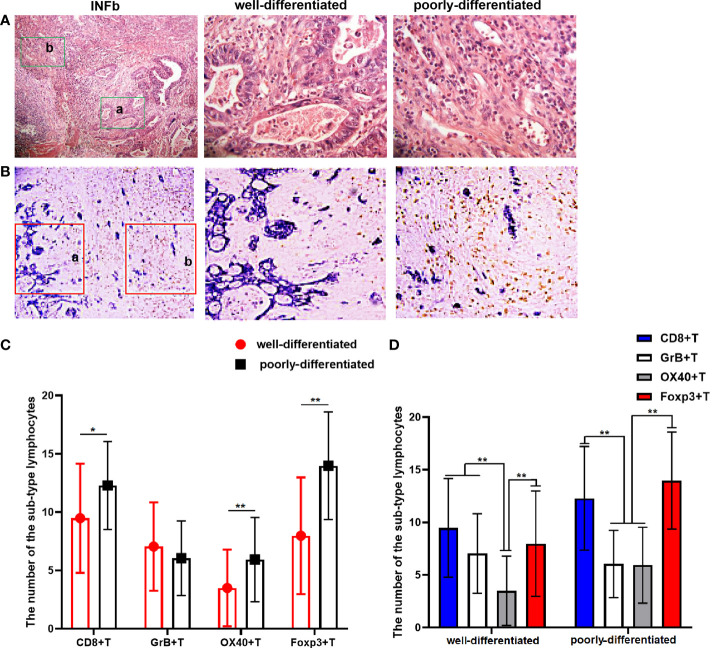
Tumor infiltration pattern (INF) and tumor origin site were reported to significantly affect the prognosis of gastric cancer (GC), while the immune status under these contexts is not clear. In this study, we correlated the density and phenotype of tumor-infiltrating lymphocytes (TILs) with INF and the tumor origin site to reflect the biological behavior of tumors from a new perspective and also determined their effects on overall survival (OS) and other related clinicopathological features in archival samples of 147 gastric cancers with 10-year follow-up data. We found that the INFc growth pattern (an invasive growth without a distinct border) of GC lacked immune cell infiltration, particularly the cytotoxic T cells and their activated form. It is also significantly associated with an unfavorable prognosis (P < 0.001) and proximal site (P = 0.001), positive lymph node metastasis (P = 0.002), and later tumor-node-metastasis stage (P < 0.001). Moreover, the density and sub-type of TILs infiltration were significantly different in disparate differentiated areas for the tumor tissue with INFb. Compared with distal gastric cancer, proximal gastric cancers were prone to grow in an INFc pattern (P = 0.001) and infiltrated with fewer TILs, experiencing a shorter survival time (P = 0.013). Multivariate analysis showed that only the INF and the density of TILs were demonstrated to be the independent prognostic factors of OS for the GC. We concluded that GC with an aggressive growth pattern arising from proximal sites always had a weak immune response and resulted in a poor prognosis. The interaction between them and their synergistic or antagonistic effects in the development of tumors need to be further studied. This study opens up a new perspective for research on the biological behavior of the tumor.
Keywords: gastric adenocarcinoma; immune status; tumor infiltration pattern; tumor origin site; tumor-infiltrating lymphocytes.
Copyright © 2022 Zhang, Wang, Hu, Zhang, Li, Zhao, Liu and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Pernot S, Terme M, Radosevic-Robin N, Castan F, Badoual C, Marcheteau E, et al. . Infiltrating and peripheral immune cell analysis in advanced gastric cancer according to the lauren classification and its prognostic significance. Gastric Cancer (2020) 23:73–81. doi: 10.1007/s10120-019-00983-3 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous