

Cervical Artery Dissections: Etiopathogenesis and Management
- PMID: 36082197
- PMCID: PMC9447449
- DOI: 10.2147/VHRM.S362844
Cervical Artery Dissections: Etiopathogenesis and Management
Abstract
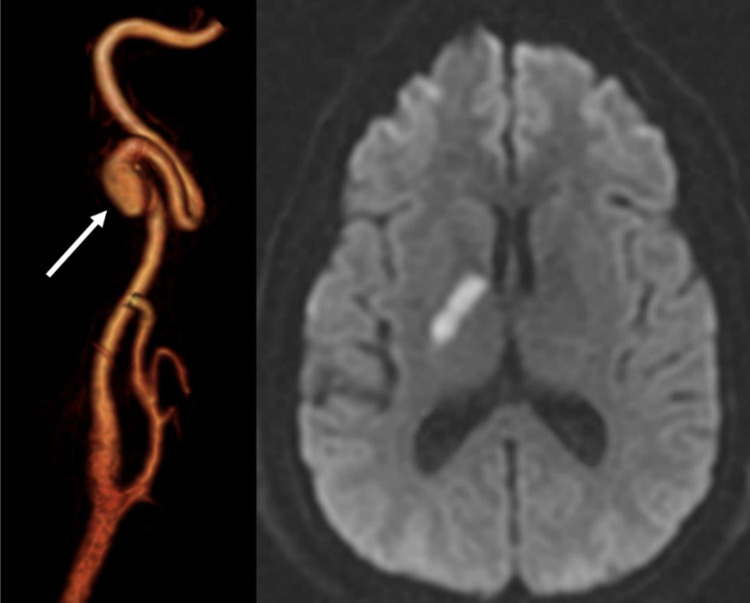
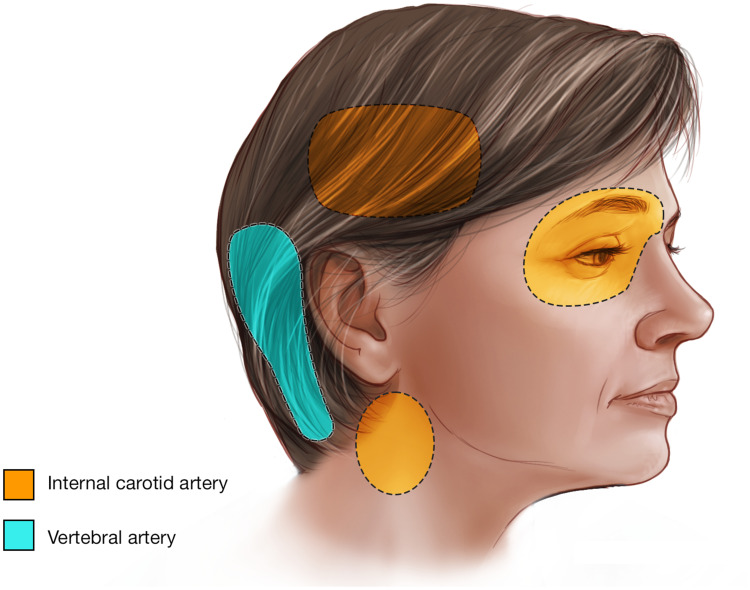
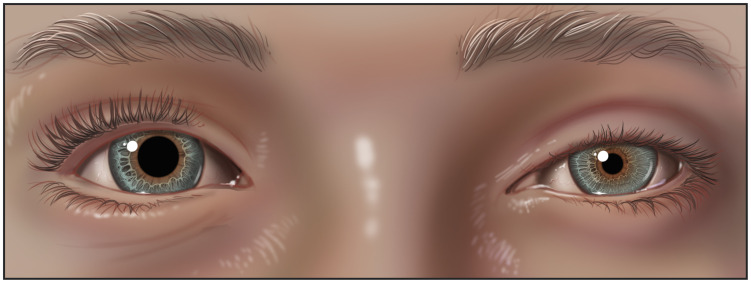
Cervical Artery Dissection (CeAD) is a frequent stroke etiology for patients younger than 50 years old. The most common immediate complications related to CeAD are headache and neck pain (65-95%), TIA/ischemic stroke (>50%), and partial Horner's syndrome (25%). The prevailing hypothesis regarding the pathogenesis of sCeAD is that the underlying constitutional vessel wall weakness of patients with sCeAD is genetically determined and that environmental factors could act as triggers. The stroke prevention treatment of CeAD remains controversial, involving anticoagulation or antiplatelet therapy and potentially emergent stenting and/or thrombectomy or angioplasty for selected cases of carotid artery dissection with occlusion. The treatment of headache associated with CeAD depends on the headache phenotype and comorbidities. Radiographically, more than 75% of CeAD cases present with occlusion or non-occlusive stenosis. Many patients demonstrate partial and complete healing, more commonly in the carotid arteries. One-fifth of the patients develop dissecting pseudoaneurysm, but this is a benign clinical entity with an extremely low rupture and stroke recurrence risk. Good recovery is achieved in many CeAD cases, and mortality remains low. Family history of CeAD, connective tissue disorders like Ehlers-Danlos syndrome type IV, and fibromuscular dysplasia are risk factors for recurrent CeAD, which can occur in 3-9% of the cases. This review serves as a comprehensive, updated overview of CeAD, emphasizing etiopathogenesis and management.
Keywords: cervical artery dissection; genetics; stroke.
© 2022 Keser et al.
Conflict of interest statement
Dr Giuseppe Lanzino reports Consultant: Superior Medical Editors: Nested Knowledge. The authors report no other conflicts of interest in this work.
Figures
References
-
- Lee VH, Brown RD, Mandrekar JN, Mokri B. Incidence and outcome of cervical artery dissection: a population-based study. Neurology. 2006;67(10):1809–1812. - PubMed
-
- Debette S, Leys D. Cervical-artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurol. 2009;8(7):668–678. - PubMed
-
- Touzé E, Gauvrit JY, Moulin T, Meder JF, Bracard S, Mas JL. Risk of stroke and recurrent dissection after a cervical artery dissection: a multicenter study. Neurology. 2003;61(10):1347–1351. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
