

European Stroke Organisation (ESO) guideline on pharmacological interventions for long-term secondary prevention after ischaemic stroke or transient ischaemic attack
- PMID: 36082250
- PMCID: PMC9446324
- DOI: 10.1177/23969873221100032
European Stroke Organisation (ESO) guideline on pharmacological interventions for long-term secondary prevention after ischaemic stroke or transient ischaemic attack
Abstract
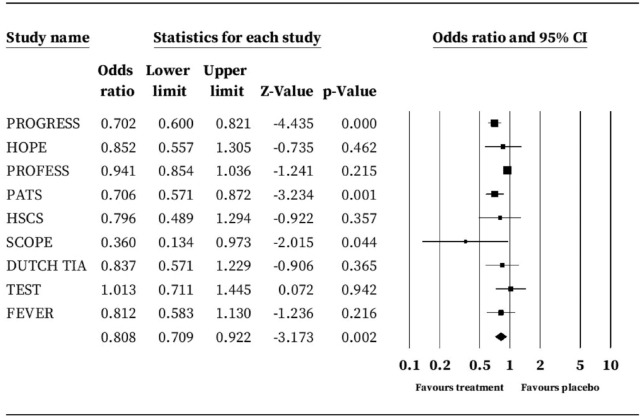
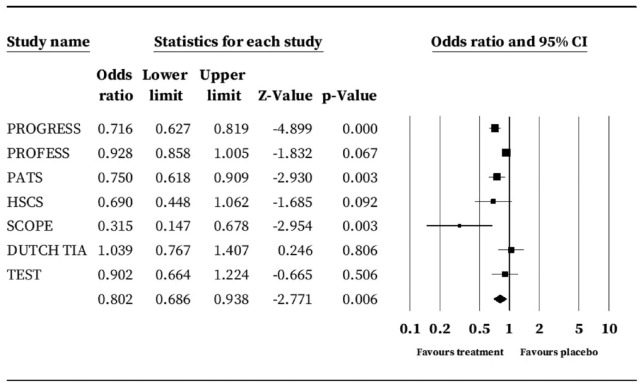
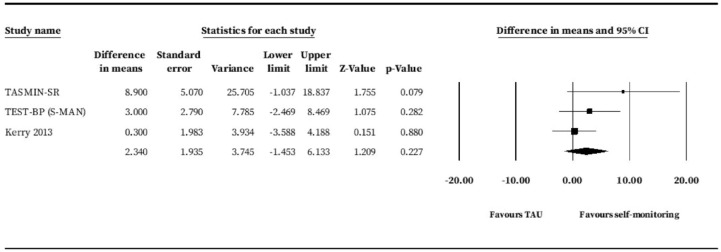
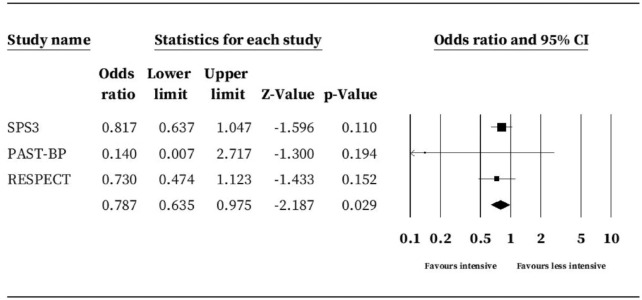
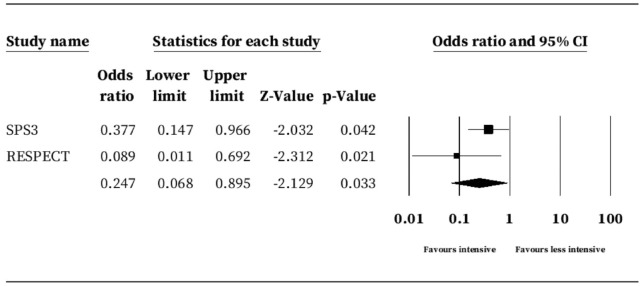
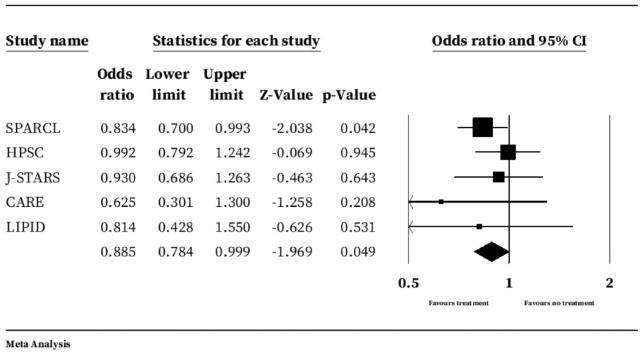
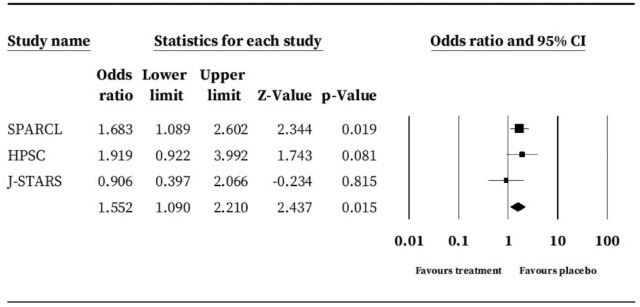
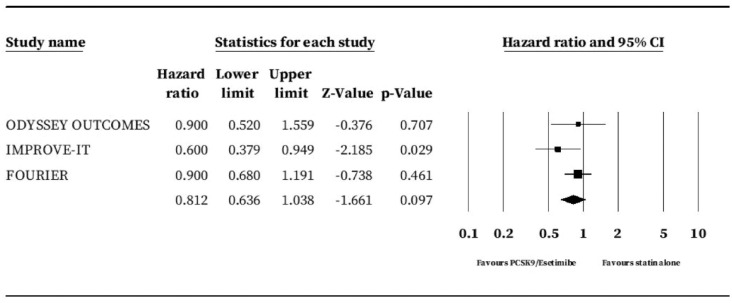
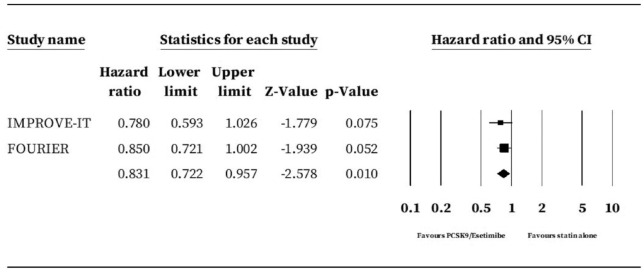
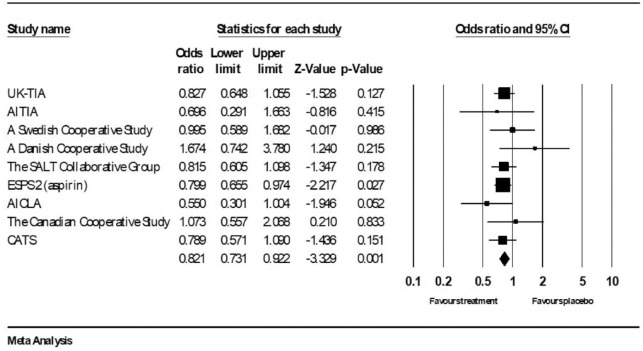
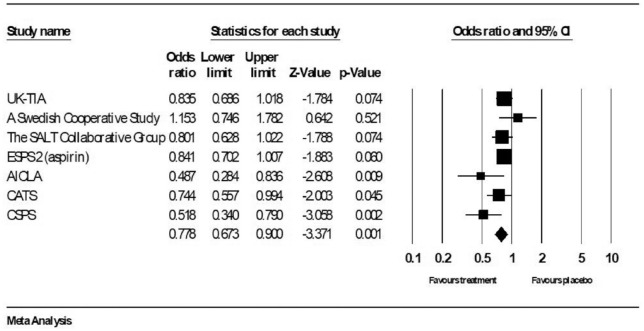
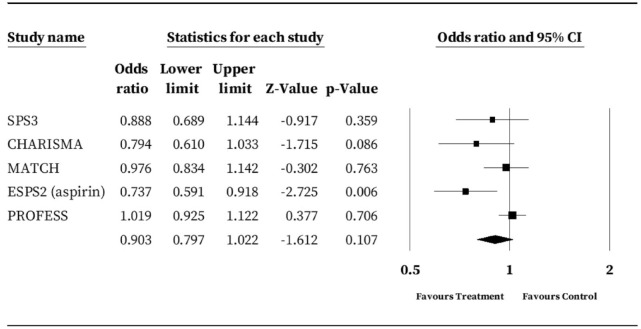
Recurrent stroke affects 9% to 15% of people within 1 year. This European Stroke Organisation (ESO) guideline provides evidence-based recommendations on pharmacological management of blood pressure (BP), diabetes mellitus, lipid levels and antiplatelet therapy for the prevention of recurrent stroke and other important outcomes in people with ischaemic stroke or transient ischaemic attack (TIA). It does not cover interventions for specific causes of stroke, including anticoagulation for cardioembolic stroke, which are addressed in other guidelines. This guideline was developed through ESO standard operating procedures and the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology. The working group identified clinical questions, selected outcomes, performed systematic reviews, with meta-analyses where appropriate, and made evidence-based recommendations, with expert consensus statements where evidence was insufficient to support a recommendation. To reduce the long-term risk of recurrent stroke or other important outcomes after ischaemic stroke or TIA, we recommend: BP lowering treatment to a target of <130/80 mmHg, except in subgroups at increased risk of harm; HMGCoA-reductase inhibitors (statins) and targeting a low density lipoprotein level of <1.8 mmol/l (70 mg/dl); avoidance of dual antiplatelet therapy with aspirin and clopidogrel after the first 90 days; to not give direct oral anticoagulant drugs (DOACs) for embolic stroke of undetermined source and to consider pioglitazone in people with diabetes or insulin resistance, after careful consideration of potential risks. In addition to the evidence-based recommendations, all or the majority of working group members supported: out-of-office BP monitoring; use of combination treatment for BP control; consideration of ezetimibe or PCSK9 inhibitors when lipid targets are not achieved; consideration of use of low-dose DOACs in addition to an antiplatelet in selected groups of people with coronary or peripheral artery disease and aiming for an HbA1c level of <53 mmol/mol (7%) in people with diabetes mellitus. These guidelines aim to standardise long-term pharmacological treatment to reduce the burden of recurrent stroke in Europe.
Keywords: Guideline; antiplatelet; diabetes; dyslipidaemia; hypertension; stroke; systematic review.
© European Stroke Organisation 2022.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed a declaration of competing interests and details are available in Supplemental Table 1.
Figures
References
-
- Béjot Y, Bailly H, Durier J, et al. Epidemiology of stroke in Europe and trends for the 21st century. Presse Med 2016; 45: e391–e398. - PubMed
-
- Rothwell PM, Coull AJ, Silver LE, et al. Population-based study of event-rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet 2005; 366: 1773–1783. - PubMed
-
- Amarenco P, Lavallée PC, Labreuche J, et al. One-year risk of stroke after transient ischemic attack or minor stroke. N Engl J Med 2016; 374: 1533–1542. - PubMed
-
- O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010; 376: 112–123. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
