

Practice effects in performance outcome measures in patients living with neurologic disorders - A systematic review
- PMID: 36082322
- PMCID: PMC9445299
- DOI: 10.1016/j.heliyon.2022.e10259
Practice effects in performance outcome measures in patients living with neurologic disorders - A systematic review
Abstract
Background: In this systematic review we sought to characterize practice effects on traditional in-clinic or digital performance outcome measures commonly used in one of four neurologic disease areas (multiple sclerosis; Huntington's disease; Parkinson's disease; and Alzheimer's disease, mild cognitive impairment and other forms of dementia), describe mitigation strategies to minimize their impact on data interpretation and identify gaps to be addressed in future work.
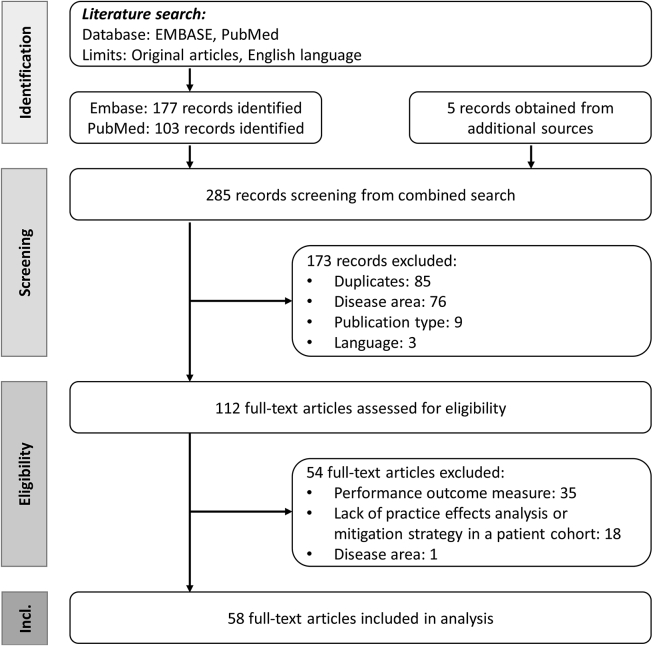
Methods: Fifty-eight original articles (49 from Embase and an additional 4 from PubMed and 5 from additional sources; cut-off date January 13, 2021) describing practice effects or their mitigation strategies were included.
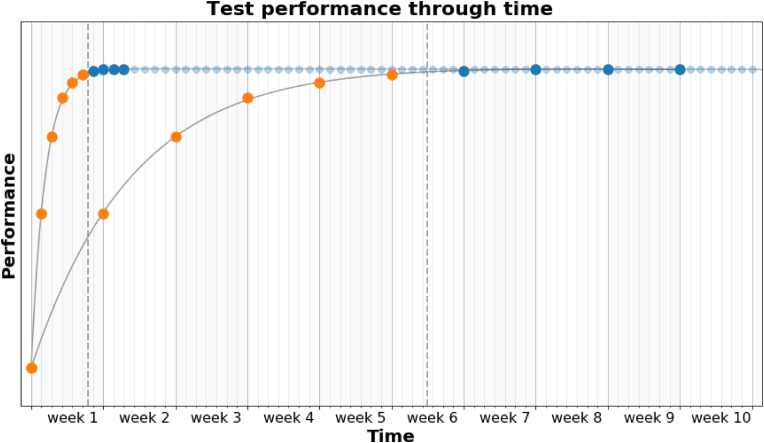
Results: Practice effects observed in healthy volunteers do not always translate to patients living with neurologic disorders. Mitigation strategies include reliable changes indices that account for practice effects or a run-in period. While the former requires data from a reference sample showing similar practice effects, the latter requires a sufficient number of tests in the run-in period to reach steady-state performance. However, many studies only included 2 or 3 test administrations, which is insufficient to define the number of tests needed in a run-in period.
Discussion: Several gaps have been identified. In particular the assessment of practice effects on an individual patient level as well as the temporal dynamics of practice effects are largely unaddressed. Here, digital tests, which allow much higher testing frequency over prolonged periods of time, can be used in future work to gain a deeper understanding of practice effects and to develop new metrics for assessing and accounting for practice effects in clinical research and clinical trials.
Keywords: Alzheimer disease; Dementia; Huntington disease; Mild cognitive impairment; Multiple sclerosis; Parkinson disease; Practice effects.
© 2022 The Author(s).
Conflict of interest statement
Sven P. Holm is a contractor for F. Hoffmann–La Roche Ltd. Arnaud M. Wolfer is an employee of F. Hoffmann–La Roche Ltd. Grégoire H.S. Pointeau is an employee and shareholder of F. Hoffmann–La Roche Ltd. Florian Lipsmeier is an employee of F. Hoffmann–La Roche Ltd. Michael Lindemann is a consultant for F. Hoffmann–La Roche Ltd. via Inovigate.
Figures
 ) indicate continuous practice effects, light green dots (
) indicate continuous practice effects, light green dots ( ) initial practice effects, yellow dots (
) initial practice effects, yellow dots ( ) inconclusive effects and red dots (
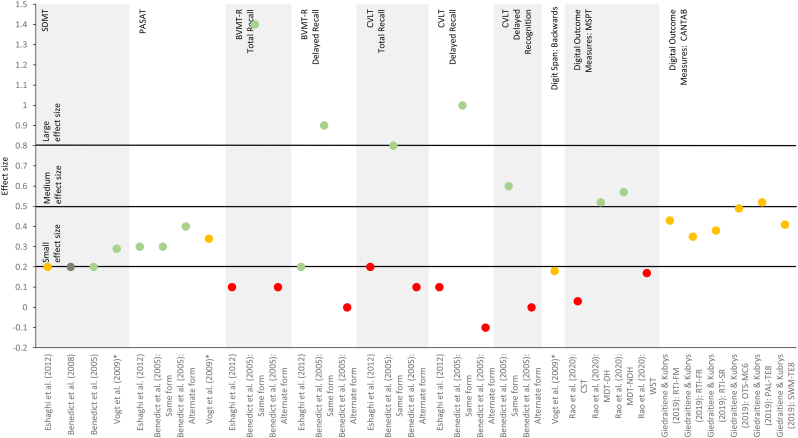
) inconclusive effects and red dots ( ) absence of practice effects, as defined in Table 4. Small, medium and large effect sizes are defined as d = 0.2, d = 0.5 and d = 0.8, respectively, and apply to Cohen's d only (Cohen, 1992). ∗ Partial η2. BVMT-R, Brief Visuospatial Memory Test-Revised; CANTAB, Cambridge Neuropsychological Test Automated Battery; CST, Contrast Sensitivity Test; CVLT, California Verbal Learning Test; MDT-DH, Dominant-handed Manual Dexterity Test; MDT-NDH, Non-dominant-handed Manual Dexterity Test; MSPT, Multiple Sclerosis Performance Test; OTS-MC6, One Touch Stockings of Cambridge with 6 moves; PAL-TE8, Total error at 8-figure stage of the Paired Associates Learning; PASAT, Paced Auditory Serial Addition Test; RTI-FM, Five-choice movement time; RTI-FR, Five-choice reaction time; RTI-SR, Simple reaction time; SDMT, Symbol Digit Modalities Test; SWM-TE8, Total error for 8 boxes of Spatial Working Memory; WST, Walking Speed Test.
) absence of practice effects, as defined in Table 4. Small, medium and large effect sizes are defined as d = 0.2, d = 0.5 and d = 0.8, respectively, and apply to Cohen's d only (Cohen, 1992). ∗ Partial η2. BVMT-R, Brief Visuospatial Memory Test-Revised; CANTAB, Cambridge Neuropsychological Test Automated Battery; CST, Contrast Sensitivity Test; CVLT, California Verbal Learning Test; MDT-DH, Dominant-handed Manual Dexterity Test; MDT-NDH, Non-dominant-handed Manual Dexterity Test; MSPT, Multiple Sclerosis Performance Test; OTS-MC6, One Touch Stockings of Cambridge with 6 moves; PAL-TE8, Total error at 8-figure stage of the Paired Associates Learning; PASAT, Paced Auditory Serial Addition Test; RTI-FM, Five-choice movement time; RTI-FR, Five-choice reaction time; RTI-SR, Simple reaction time; SDMT, Symbol Digit Modalities Test; SWM-TE8, Total error for 8 boxes of Spatial Working Memory; WST, Walking Speed Test.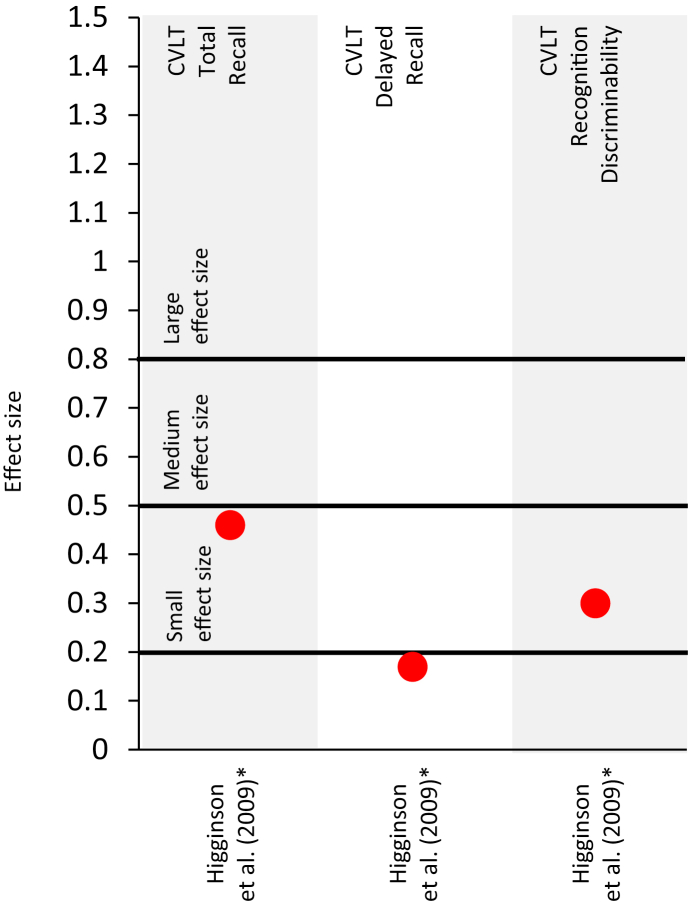 ) absence of practice effects, as defined in Table 5. Small, medium and large effect sizes are defined as d = 0.2, d = 0.5 and d = 0.8, respectively (Cohen, 1992). CVLT, California Verbal Learning Test. ∗Effect size indicates a worsening in test performance.
) absence of practice effects, as defined in Table 5. Small, medium and large effect sizes are defined as d = 0.2, d = 0.5 and d = 0.8, respectively (Cohen, 1992). CVLT, California Verbal Learning Test. ∗Effect size indicates a worsening in test performance.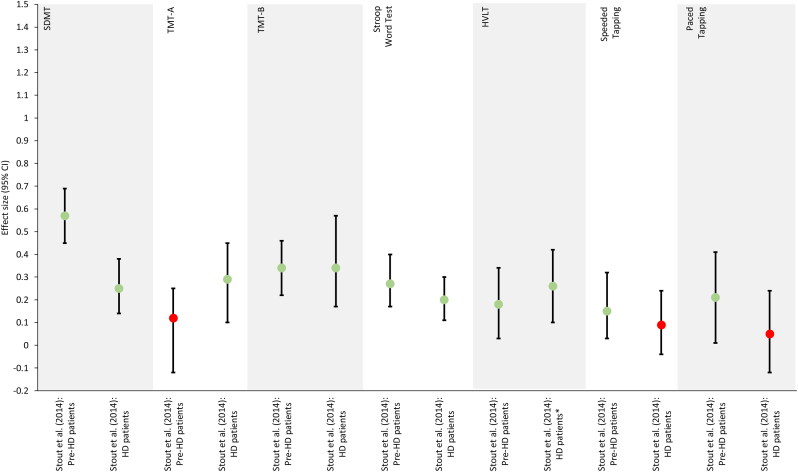 ) indicate initial practice effects. Red dots () indicate an absence of practice effects, as defined in Table 6. ∗ Effect size reported for the change observed between the second and third test iteration rather than between the first and second test iteration. CVLT, California Verbal Learning Test; HD, Huntington's disease; HVLT, Hopkins Verbal Learning Test; pre-HD, pre-manifest Huntington's disease; SDMT, Symbol Digit Modalities Test; TMT, Trail-Making Test.
) indicate initial practice effects. Red dots () indicate an absence of practice effects, as defined in Table 6. ∗ Effect size reported for the change observed between the second and third test iteration rather than between the first and second test iteration. CVLT, California Verbal Learning Test; HD, Huntington's disease; HVLT, Hopkins Verbal Learning Test; pre-HD, pre-manifest Huntington's disease; SDMT, Symbol Digit Modalities Test; TMT, Trail-Making Test.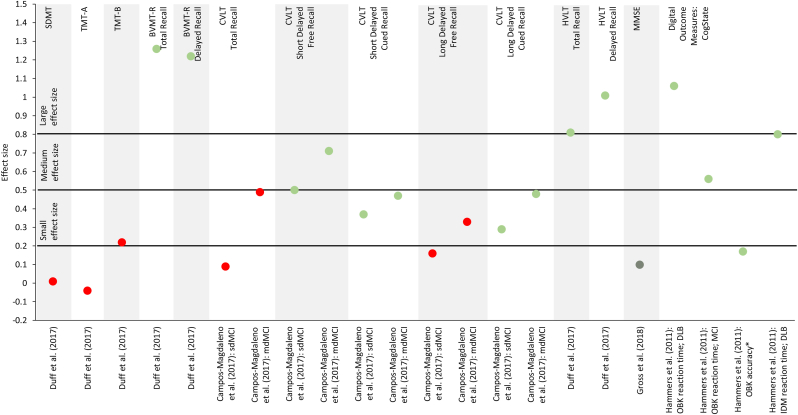 ) indicate continuous practice effects, light green dots () initial practice effects, yellow dots () inconclusive effects and red dots () absence of practice effects, as defined in Table 7. Small, medium and large effect sizes are defined as d = 0.2, d = 0.5 and d = 0.8, respectively, and apply to Cohen's d only (Cohen, 1992). ∗η2. BVMT-R, Brief Visuospatial Memory Test-Revised; CVLT, California Verbal Learning Test; DLB, dementia with Lewis bodies; HVLT, Hopkins Verbal Learning Test; IDM, divided attention task; LDFR, long delayed free recall; LM, Logical Memory; LNS, Letter-Number Sequencing; MCI, mild cognitive impairment; mdMCI, multi-domain mild cognitive impairment; MMSE, Mini-Mental State Examination; OBK, One-Back Test; SDFR, short delayed free recall; sdMCI, single-domain mild cognitive impairment; SDMT, Symbol Digit Modalities Test; TMT, Trail-Making Test; TR, total recall; VR, Visual Reproduction; WAIS, Wechsler Adult Intelligence Scale; WMS, Wechsler Memory Scale.
) indicate continuous practice effects, light green dots () initial practice effects, yellow dots () inconclusive effects and red dots () absence of practice effects, as defined in Table 7. Small, medium and large effect sizes are defined as d = 0.2, d = 0.5 and d = 0.8, respectively, and apply to Cohen's d only (Cohen, 1992). ∗η2. BVMT-R, Brief Visuospatial Memory Test-Revised; CVLT, California Verbal Learning Test; DLB, dementia with Lewis bodies; HVLT, Hopkins Verbal Learning Test; IDM, divided attention task; LDFR, long delayed free recall; LM, Logical Memory; LNS, Letter-Number Sequencing; MCI, mild cognitive impairment; mdMCI, multi-domain mild cognitive impairment; MMSE, Mini-Mental State Examination; OBK, One-Back Test; SDFR, short delayed free recall; sdMCI, single-domain mild cognitive impairment; SDMT, Symbol Digit Modalities Test; TMT, Trail-Making Test; TR, total recall; VR, Visual Reproduction; WAIS, Wechsler Adult Intelligence Scale; WMS, Wechsler Memory Scale.References
-
- Bachoud-Lévi A.C., Maison P., Bartolomeo P., Boissé M.F., Dalla Barba G., Ergis A.M., Baudic S., Degos J.D., Cesaro P., Peschanski M. Retest effects and cognitive decline in longitudinal follow-up of patients with early HD. Neurology. 2001;56:1052–1058. - PubMed
-
- Barker-Collo S.L. Within session practice effects on the PASAT in clients with multiple sclerosis. Arch. Clin. Neuropsychol. 2005;20:145–152. - PubMed
-
- Beglinger L.J., Adams W.H., Langbehn D., Fiedorowicz J.G., Caviness J., Biglan K., Olson B., Paulsen J.S. Does interval between screening and baseline matter in HD cognitive clinical trials? J Huntingtons Dis. 2014;3:139–144. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
