

Multicenter comparative study of open, laparoscopic, and robotic pyeloplasty in the pediatric population for the treatment of ureteropelvic junction obstruction (UPJO)
- PMID: 36083265
- PMCID: PMC9747029
- DOI: 10.1590/S1677-5538.IBJU.2022.0194
Multicenter comparative study of open, laparoscopic, and robotic pyeloplasty in the pediatric population for the treatment of ureteropelvic junction obstruction (UPJO)
Abstract
Introduction: Dismembered open pyeloplasty described by Anderson and Hynes is the "gold standard" for the treatment of ureteropelvic junction obstruction. The aim of our study was to compare the results of open (OP) vs laparoscopic (LP) vs robotic (RALP) pyeloplasty.
Material and methods: A multicenter prospective review was conducted of pyeloplasty surgeries performed at five high-volume centers between 2014 and 2018. Demographic data, history of prenatal hydronephrosis, access type, MAG3 renogram and differential renal function, surgery time, length of hospital stay, and complication rate (Clavien-Dindo) were recorded. Access type was compared using the Kruskal-Wallis, Chi-square, or Fisher's exact tests.
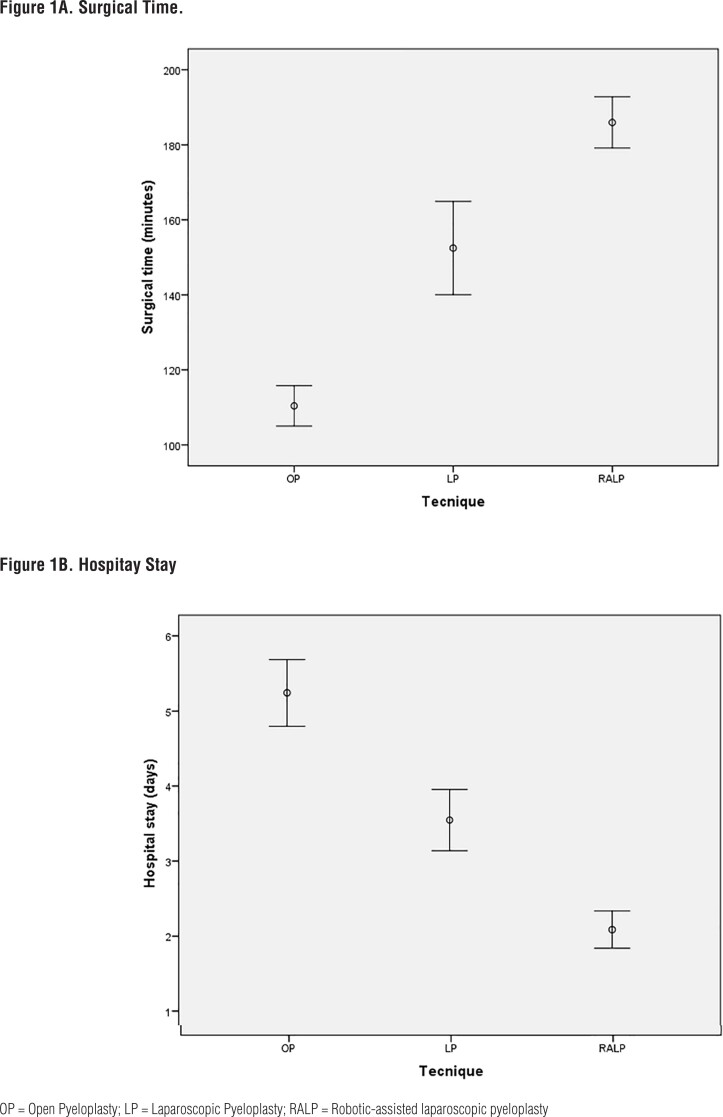
Results: A total of 322 patients were included: 62 OP, 86 LP, and 174 RALP. The mean age was 8.13 (r: 1-16) years, with a statistically significant lower age (mean 5 years) in OP (p < 0.001). There were no significant differences in the distribution of the side affected. Operative time was 110.5 min for OP, 140 min for LP, and 179 min for RALP (p < 0.0001). Hospital stay was significantly shorter in the RALP group than in the other groups (p < 0.0001). There were no differences in postoperative complications and reoperations between the three groups.
Conclusions: Minimally invasive surgery for the management of UPJO in children is gaining more acceptance, even in patients younger than 1-year-old. Operative time continues to be significantly shorter in OP than in LP and RALP. Hospital stay was shorter in RALP compared to the other techniques. No differences were found in complication rates, type of complications, and reoperation rate.
Keywords: Laparoscopy; Robotics; Ureteral Obstruction.
Copyright® by the International Brazilian Journal of Urology.
Conflict of interest statement
None declared.
Figures
Comment in
-
Minimally invasive surgery for pyeloplasty poised to become The preferred surgical technique irrespective of age.Int Braz J Urol. 2022 Nov-Dec;48(6):969-970. doi: 10.1590/S1677-5538.IBJU.2022.0194.1. Int Braz J Urol. 2022. PMID: 36173408 Free PMC article. No abstract available.
References
-
- Anderson JC, Hynes W. Retrocaval ureter; a case diagnosed pre-operatively and treated successfully by a plastic operation. Br J Urol. 1949;21:209–214. - PubMed
-
- O’Reilly PH, Brooman PJ, Mak S, Jones M, Pickup C, Atkinson C, et al. The long-term results of Anderson-Hynes pyeloplasty. BJU Int. 2001;87:287–289. - PubMed
-
- Peters CA, Schlussel RN, Retik AB. Pediatric laparoscopic dismembered pyeloplasty. J Urol. 1995;153:1962–1965. - PubMed
-
- Mei H, Pu J, Yang C, Zhang H, Zheng L, Tong Q. Laparoscopic versus open pyeloplasty for ureteropelvic junction obstruction in children: a systematic review and meta-analysis. J Endourol. 2011;25:727–736. - PubMed
-
- Tan HL, Roberts JP. Laparoscopic dismembered pyeloplasty in children: preliminary results. Br J Urol. 1996;77:909–913. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous