

Interstitial Lung Abnormalities at CT: Subtypes, Clinical Significance, and Associations with Lung Cancer
- PMID: 36083805
- PMCID: PMC9630713
- DOI: 10.1148/rg.220073
Interstitial Lung Abnormalities at CT: Subtypes, Clinical Significance, and Associations with Lung Cancer
Abstract
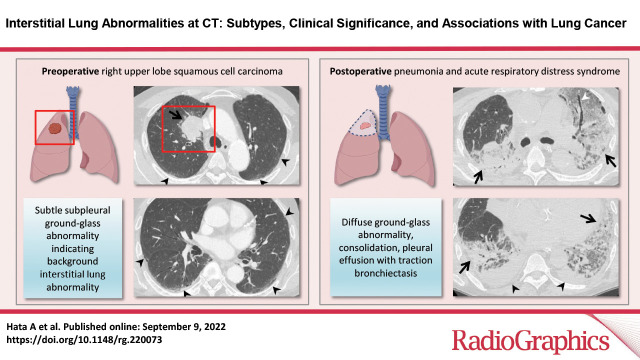
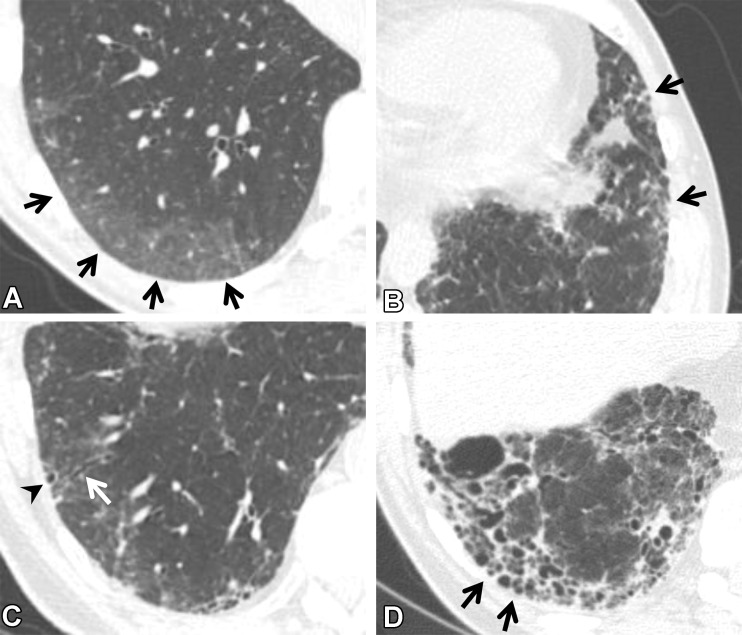
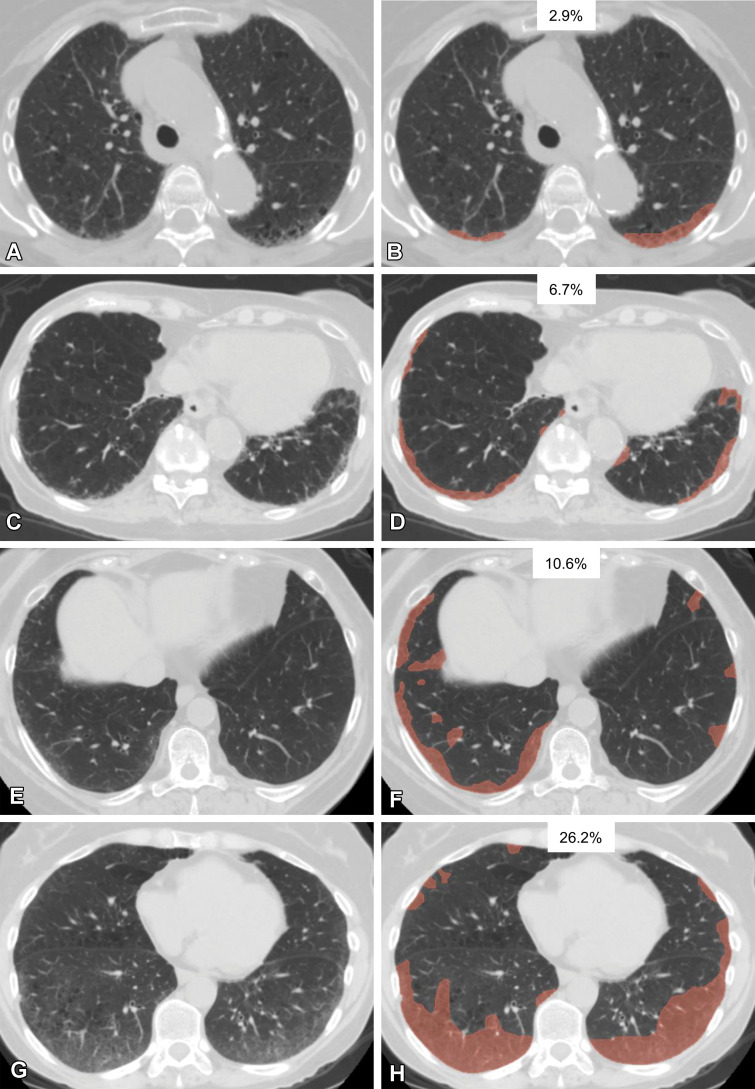
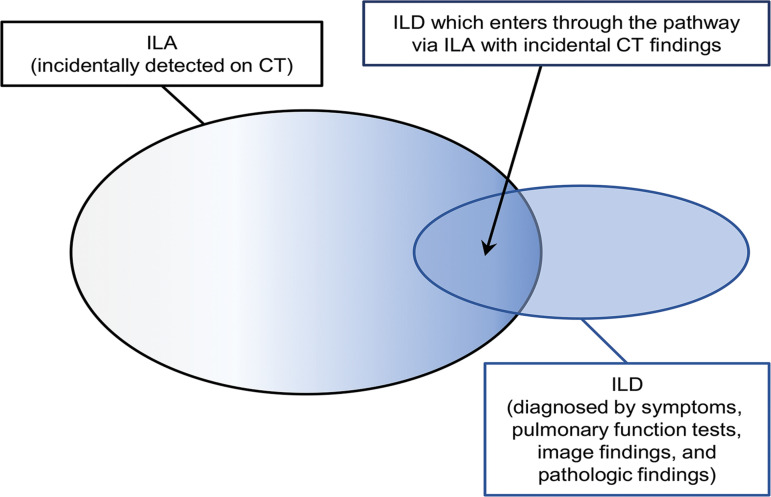
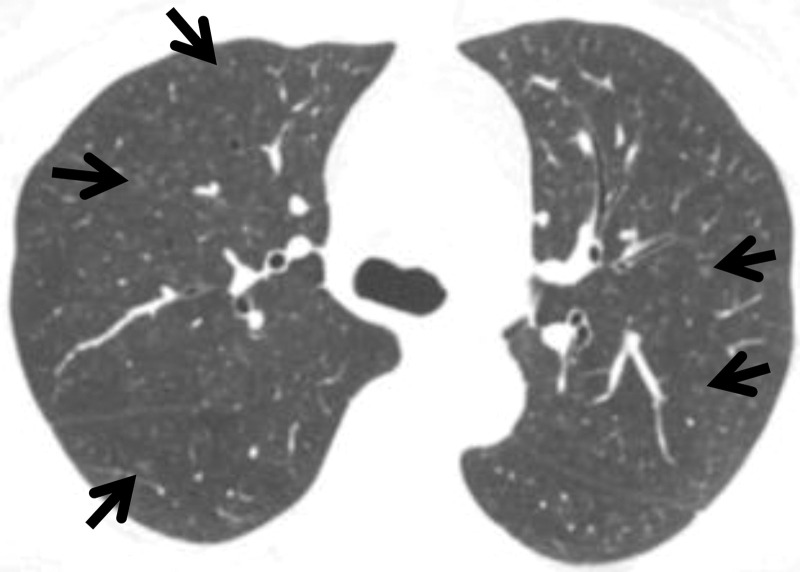
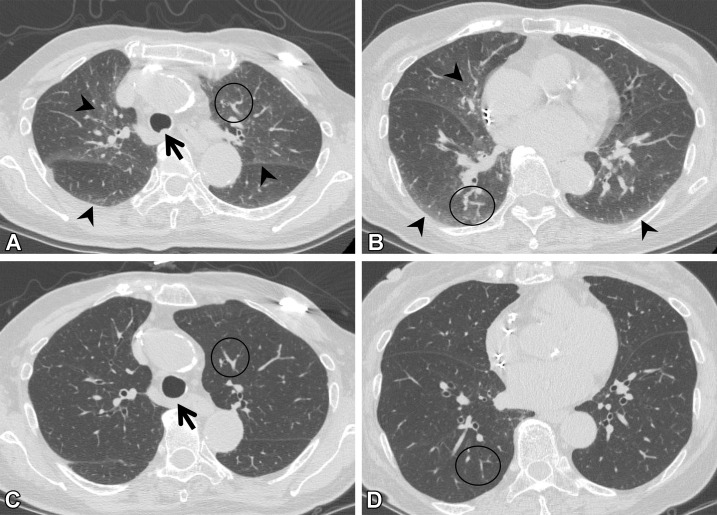
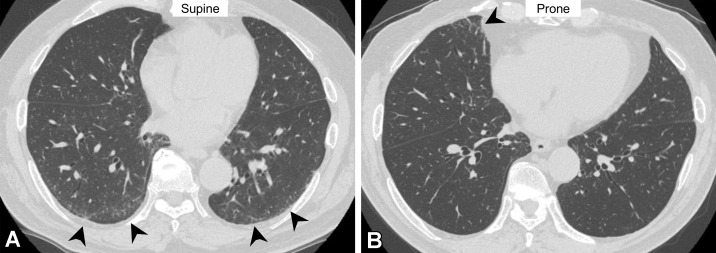
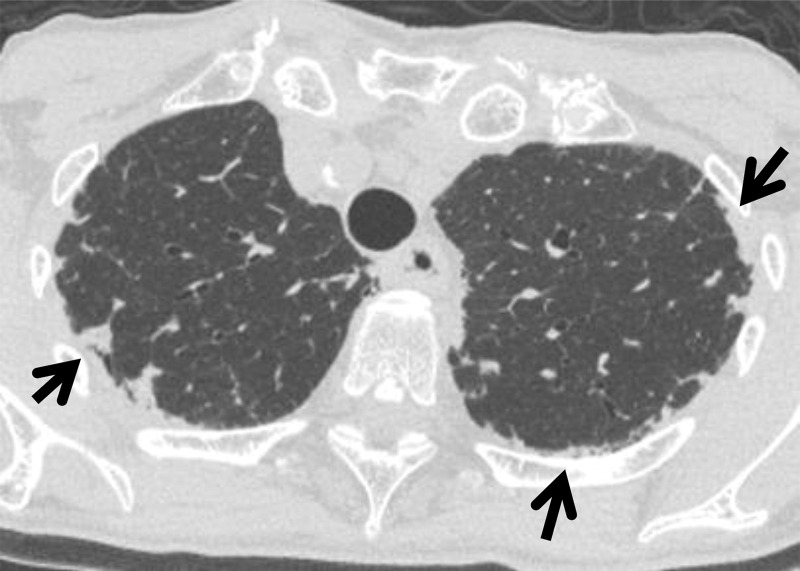
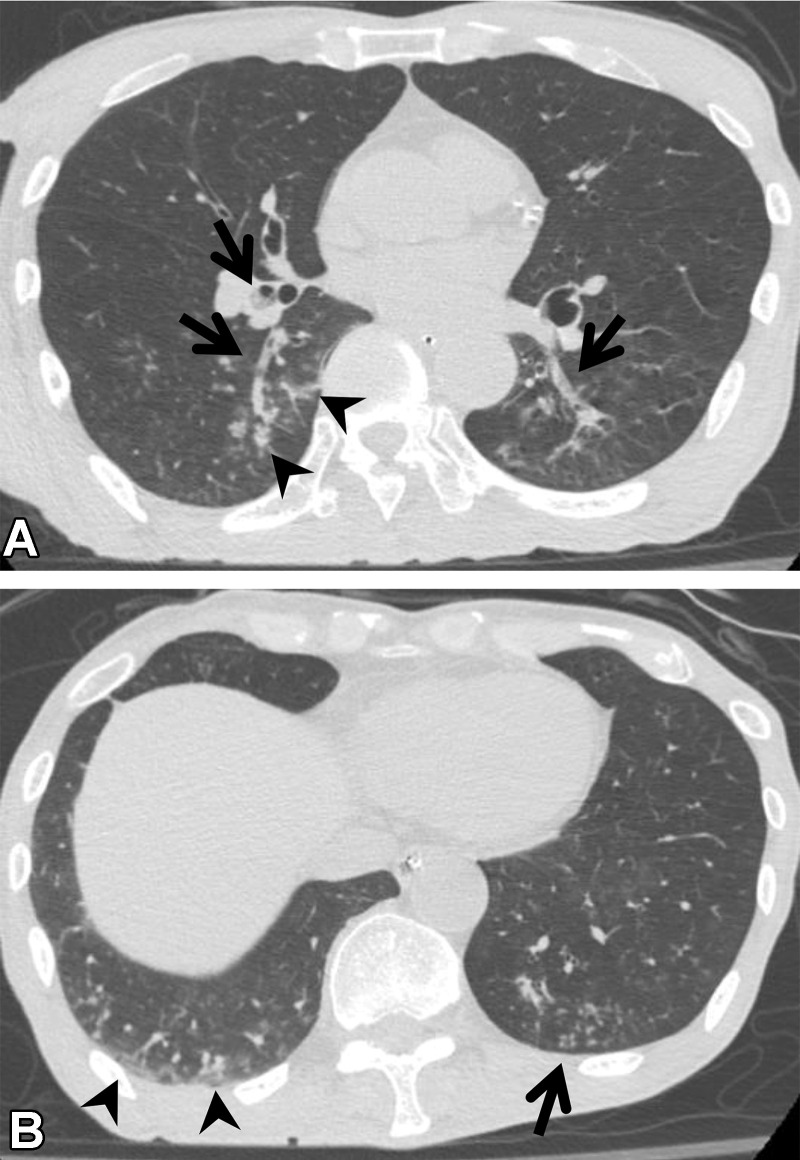
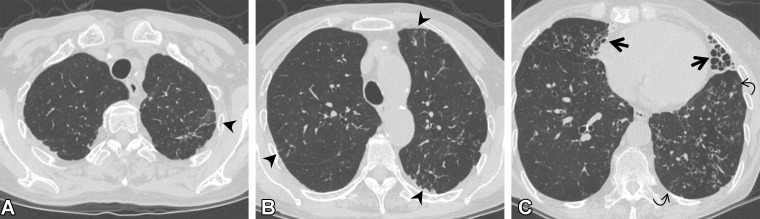
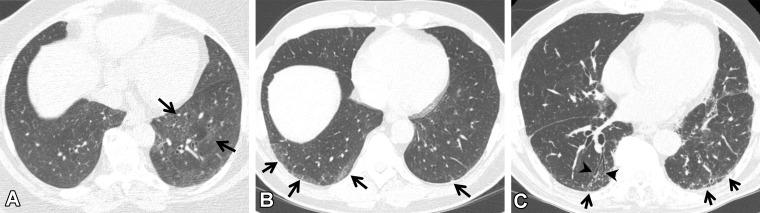
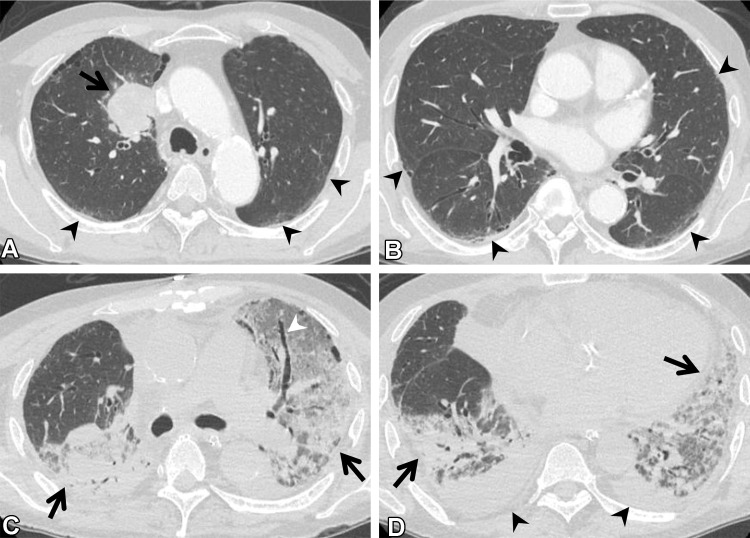
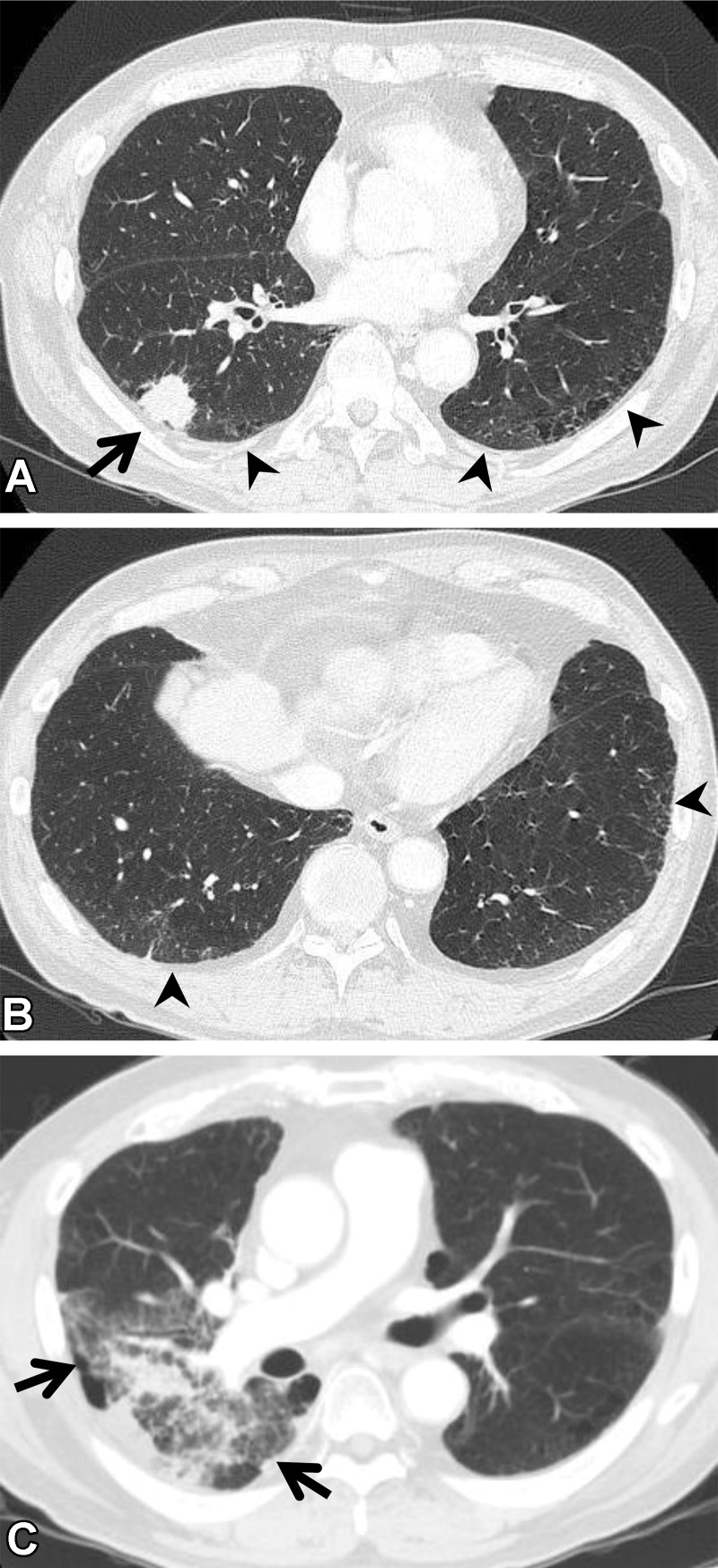
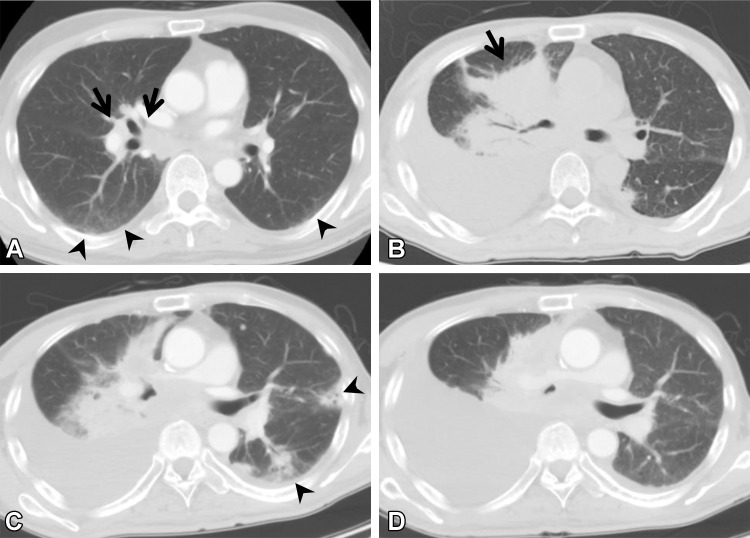
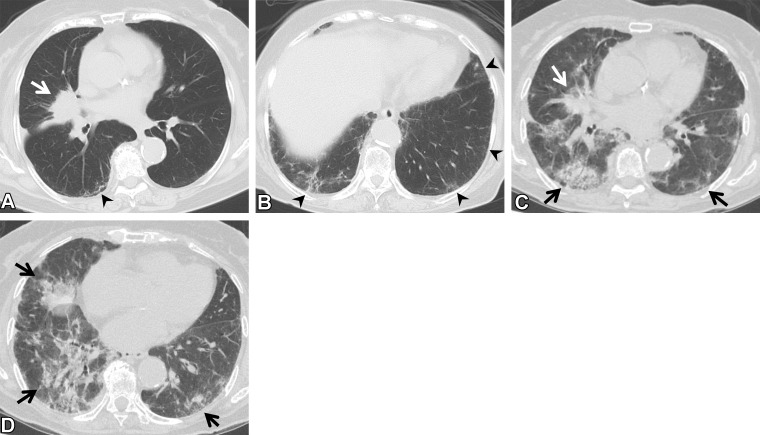
Interstitial lung abnormality (ILA) is defined as an interstitial change detected incidentally on CT images. It is seen in 4%-9% of smokers and 2%-7% of nonsmokers. ILA has a tendency to progress with time and is associated with respiratory symptoms, decreased exercise capability, reduced pulmonary function, and increased mortality. ILAs can be classified into three subcategories: nonsubpleural, subpleural nonfibrotic, and subpleural fibrotic. In cases of ILA, clinically significant interstitial lung disease should be identified and requires clinically driven management by a pulmonologist. Risk factors for the progression of ILA include clinical elements (ie, inhalation exposures, medication use, radiation therapy, thoracic surgery, physiologic findings, and gas exchange findings) and radiologic elements (ie, basal and peripheral predominance and fibrotic findings). It is recommended that individuals with one or more clinical or radiologic risk factors for progression of ILA be actively monitored with pulmonary function testing and CT. To avoid overcalling ILA at CT, radiologists must recognize the imaging pitfalls, including centrilobular nodularity, dependent abnormality, suboptimal inspiration, osteophyte-related lesions, apical cap and pleuroparenchymal fibroelastosis-like lesions, aspiration, and infection. There is a close association between ILA and lung cancer, and many studies have reported an increased incidence of lung cancer, worse prognoses, and/or increased pulmonary complications in relation to cancer treatment in patients with ILA. ILA is considered to be an important comorbidity in patients with lung cancer. Accordingly, all radiologists involved with body CT must have sound knowledge of ILAs owing to the high prevalence and potential clinical significance of these anomalies. An overview of ILAs, including a literature review of the associations between ILAs and lung cancer, is presented. ©RSNA, 2022.
Conflict of interest statement
Figures

References
-
- Hatabu H , Hunninghake GM , Lynch DA . Interstitial lung abnormality: recognition and perspectives . Radiology 2019. ; 291 ( 1 ): 1 – 3 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
