

Development of lab score system for predicting COVID-19 patient severity: A retrospective analysis
- PMID: 36084080
- PMCID: PMC9462772
- DOI: 10.1371/journal.pone.0273006
Development of lab score system for predicting COVID-19 patient severity: A retrospective analysis
Abstract
Aim: To develop an accurate lab score based on in-hospital patients' potent clinical and biological parameters for predicting COVID-19 patient severity during hospital admission.
Methods: To conduct this retrospective analysis, a derivation cohort was constructed by including all the available biological and clinical parameters of 355 COVID positive patients (recovered = 285, deceased = 70), collected in November 2020-September 2021. For identifying potent biomarkers and clinical parameters to determine hospital admitted patient severity or mortality, the receiver operating characteristics (ROC) curve and Fischer's test analysis was performed. Relative risk regression was estimated to develop laboratory scores for each clinical and routine biological parameter. Lab score was further validated by ROC curve analysis of the validation cohort which was built with 50 COVID positive hospital patients, admitted during October 2021-January 2022.
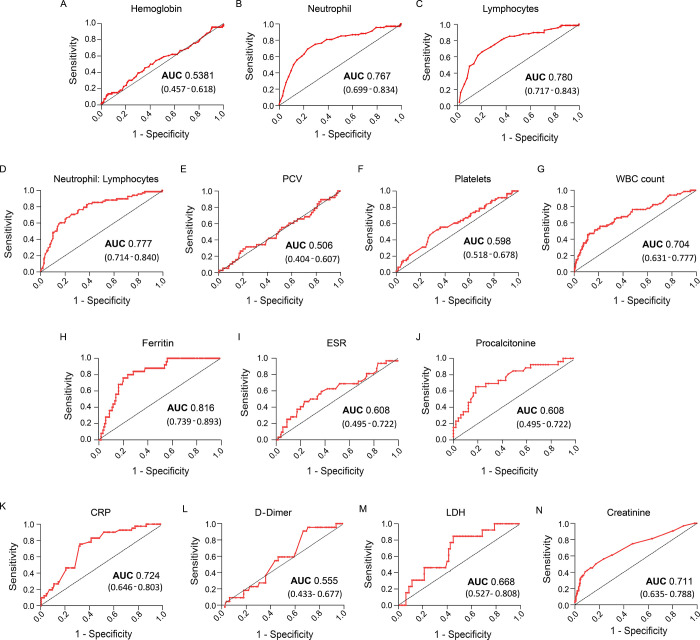
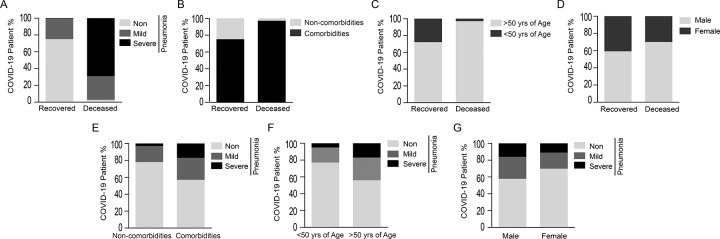
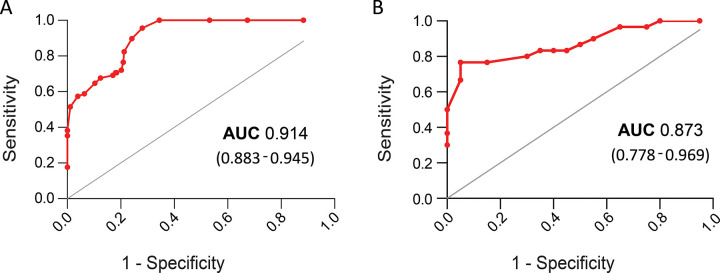
Results: Sensitivity vs. 1-specificity ROC curve (>0.7 Area Under the Curve, 95% CI) and univariate analysis (p<0.0001) of the derivation cohort identified five routine biomarkers (neutrophil, lymphocytes, neutrophil: lymphocytes, WBC count, ferritin) and three clinical parameters (patient age, pre-existing comorbidities, admitted with pneumonia) for the novel lab score development. Depending on the relative risk (p values and 95% CI) these clinical parameters were scored and attributed to both the derivation cohort (n = 355) and the validation cohort (n = 50). ROC curve analysis estimated the Area Under the Curve (AUC) of the derivation and validation cohort which was 0.914 (0.883-0.945, 95% CI) and 0.873 (0.778-0.969, 95% CI) respectively.
Conclusion: The development of proper lab scores, based on patients' clinical parameters and routine biomarkers, would help physicians to predict patient risk at the time of their hospital admission and may improve hospital-admitted COVID-19 patients' survivability.
Conflict of interest statement
No. The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
