

A multi-disciplinary, comprehensive approach to management of children with heterotaxy
- PMID: 36085154
- PMCID: PMC9463860
- DOI: 10.1186/s13023-022-02515-2
A multi-disciplinary, comprehensive approach to management of children with heterotaxy
Abstract
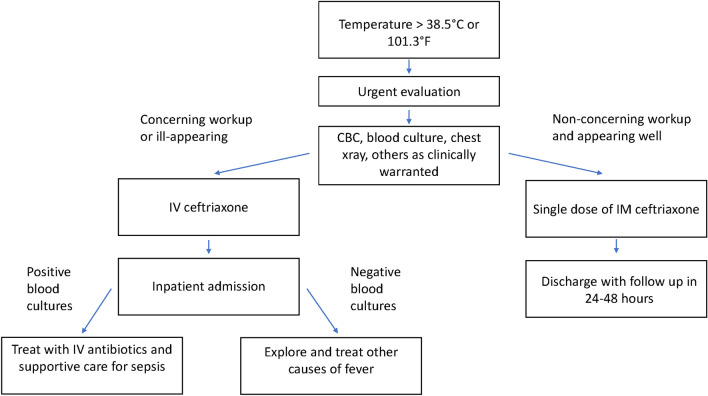
Heterotaxy (HTX) is a rare condition of abnormal thoraco-abdominal organ arrangement across the left-right axis of the body. The pathogenesis of HTX includes a derangement of the complex signaling at the left-right organizer early in embryogenesis involving motile and non-motile cilia. It can be inherited as a single-gene disorder, a phenotypic feature of a known genetic syndrome or without any clear genetic etiology. Most patients with HTX have complex cardiovascular malformations requiring surgical intervention. Surgical risks are relatively high due to several serious comorbidities often seen in patients with HTX. Asplenia or functional hyposplenism significantly increase the risk for sepsis and therefore require antimicrobial prophylaxis and immediate medical attention with fever. Intestinal rotation abnormalities are common among patients with HTX, although volvulus is rare and surgical correction carries substantial risk. While routine screening for intestinal malrotation is not recommended, providers and families should promptly address symptoms concerning for volvulus and biliary atresia, another serious morbidity more common among patients with HTX. Many patients with HTX have chronic lung disease and should be screened for primary ciliary dyskinesia, a condition of respiratory cilia impairment leading to bronchiectasis. Mental health and neurodevelopmental conditions need to be carefully considered among this population of patients living with a substantial medical burden. Optimal care of children with HTX requires a cohesive team of primary care providers and experienced subspecialists collaborating to provide compassionate, standardized and evidence-based care. In this statement, subspecialty experts experienced in HTX care and research collaborated to provide expert- and evidence-based suggestions addressing the numerous medical issues affecting children living with HTX.
Keywords: Asplenia; Congenital heart disease; Heterotaxy; Laterality disorder.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests in this section.
Figures



References
-
- Tan YW, Khalil A, Kakade M, Carvalho JS, Bradley S, Cleeve S, et al. Screening and treatment of intestinal rotational abnormalities in heterotaxy: a systematic review and meta-analysis. J Pediatr. 2016;171(153–62):e1–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
