

Levoketoconazole in the treatment of patients with endogenous Cushing's syndrome: a double-blind, placebo-controlled, randomized withdrawal study (LOGICS)
- PMID: 36085339
- PMCID: PMC9675660
- DOI: 10.1007/s11102-022-01263-7
Levoketoconazole in the treatment of patients with endogenous Cushing's syndrome: a double-blind, placebo-controlled, randomized withdrawal study (LOGICS)
Abstract
Purpose: The efficacy of levoketoconazole for endogenous Cushing's syndrome was demonstrated in a phase 3, open-label study (SONICS). This study (LOGICS) evaluated drug-specificity of cortisol normalization.
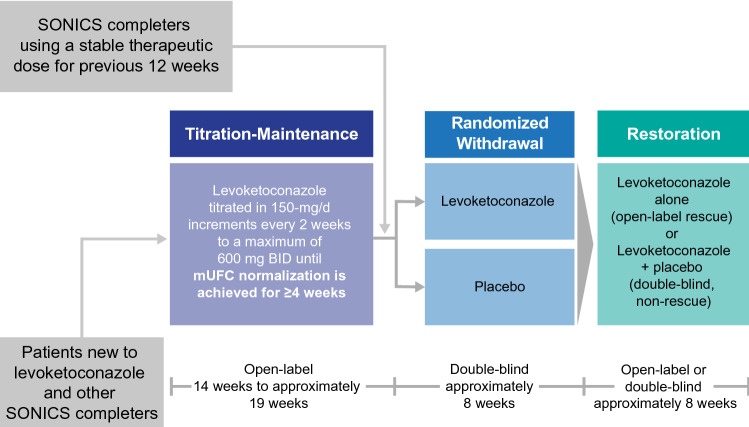
Methods: LOGICS was a phase 3, placebo-controlled, randomized-withdrawal study with open-label titration-maintenance (14-19 weeks) followed by double-blind, randomized-withdrawal (~ 8 weeks), and restoration (~ 8 weeks) phases.
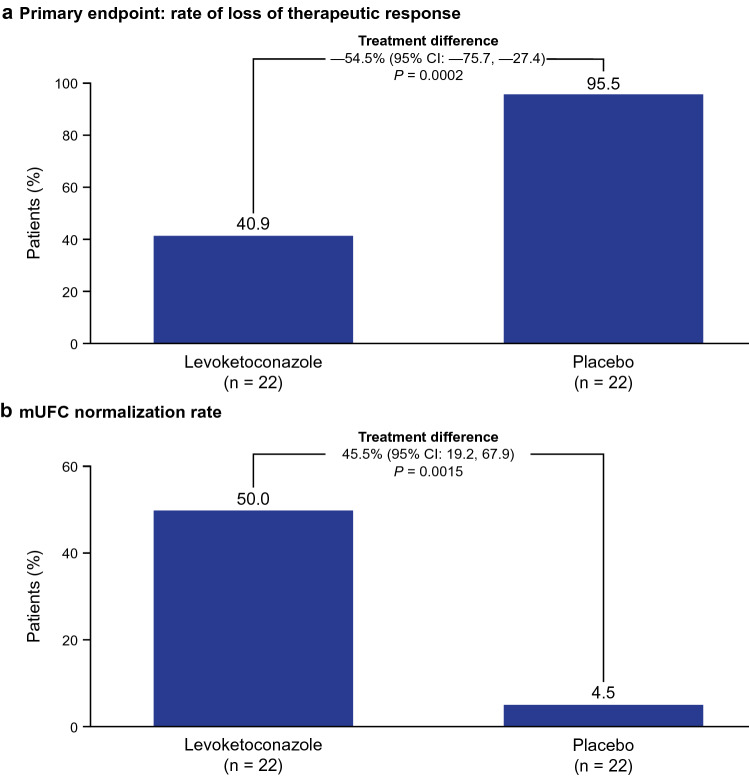
Results: 79 patients received levoketoconazole during titration-maintenance; 39 patients on a stable dose (~ 4 weeks or more) proceeded to randomization. These and 5 SONICS completers who did not require dose titration were randomized to levoketoconazole (n = 22) or placebo (n = 22). All patients with loss of response (the primary endpoint) met the prespecified criterion of mean urinary free cortisol (mUFC) > 1.5 × upper limit of normal. During randomized-withdrawal, 21 patients withdrawn to placebo (95.5%) lost mUFC response compared with 9 patients continuing levoketoconazole (40.9%); treatment difference: - 54.5% (95% CI - 75.7, - 27.4; P = 0.0002). At the end of randomized-withdrawal, mUFC normalization was observed among 11 (50.0%) patients receiving levoketoconazole and 1 (4.5%) receiving placebo; treatment difference: 45.5% (95% CI 19.2, 67.9; P = 0.0015). Restoration of levoketoconazole reversed loss of cortisol control in most patients who had received placebo. Adverse events were reported in 89% of patients during treatment with levoketoconazole (dose-titration, randomized-withdrawal, and restoration phases combined), most commonly nausea (29%) and hypokalemia (26%). Prespecified adverse events of special interest with levoketoconazole were liver-related (10.7%), QT interval prolongation (10.7%), and adrenal insufficiency (9.5%).
Conclusions: Levoketoconazole reversibly normalized urinary cortisol in patients with Cushing's syndrome. No new risks of levoketoconazole treatment were identified.
Keywords: Cushing’s disease; Cushing’s syndrome; Hypercortisolism; Levoketoconazole; Placebo; Steroidogenesis inhibitor.
© 2022. The Author(s).
Conflict of interest statement
RP reports receiving research support to Federico II University of Naples as a principal investigator for clinical trials from Corcept Therapeutics, HRA Pharma, Novartis, Recordati, and Xeris Biopharma/Strongbridge Biopharma; receiving different research support to Federico II University of Naples from Novartis and Xeris/Strongbridge; and receiving occassional consulting honoraria from Corcept Therapeutics, HRA Pharma, Novartis, Recordati, and Xeris/Strongbridge. SZ reports receiving consulting honoraria from Novartis. AE reports serving as the principal investigator/sub-investigator of clinical trials for Corcept Therapeutics and Novartis; and receiving consulting honoraria from Novartis. MT reports serving as the principal investigator of clinical trials for Corcept Therapeutics, HRA Pharma, Novartis, and Xeris/Strongbridge; serving as an occasional scientific consultant to HRA Pharma and Recordati; and receiving speaker’s fees from Medis, Novartis, and Xeris/Strongbridge. IS reports receiving research grants, consulting, and lectureship fees from Medison Pharma, Novartis International, and Pfizer. AS reports receiving no grants or consulting honoraria from pharmaceutical companies. CB reports serving as the principal investigator of research grants from Novo Nordisk and Xeris/Strongbridge; and receiving consulting honoraria from Ipsen. TB reports serving as a clinical trial investigator for Novartis and Xeris/Strongbridge; receiving research grants from Ipsen and Pfizer; and serving as an advisory board member or receiving speaker’s fees from Ipsen, Novartis, Pfizer, and Xeris/Strongbridge. CEG reports serving as the principal investigator of clinical trials for HRA Pharma and Xeris/Strongbridge. ST reports receiving research and travel grants and consulting honoraria from Novartis; and receiving consulting honoraria from Recordati. FC is a former employee of Strongbridge Biopharma/Xeris Pharma and reports receiving consulting fees from Xeris. MF reports serving as an investigator with research grants to OHSU from Novartis, Recordati, and Xeris/Strongbridge; serving as an occasional scientific consultant to HRA Pharma, Recordati, Sparrow, and Xeris/Strongbridge; and is on the Editorial Board of Pituitary.
Figures


References
-
- Andela CD, van Haalen FM, Ragnarsson O, Papakokkinou E, Johannsson G, Santos A, Webb SM, Biermasz NR, van der Wee NJ, Pereira AM. Mechanisms in endocrinology: Cushing's syndrome causes irreversible effects on the human brain: a systematic review of structural and functional magnetic resonance imaging studies. Eur J Endocrinol. 2015;173(1):R1–R14. doi: 10.1530/EJE-14-1101. - DOI - PubMed
-
- Ragnarsson O, Olsson DS, Papakokkinou E, Chantzichristos D, Dahlqvist P, Segerstedt E, Olsson T, Petersson M, Berinder K, Bensing S, Höybye C, Edén-Engström B, Burman P, Bonelli L, Follin C, Petranek D, Erfurth EM, Wahlberg J, Ekman B, Åkerman AK, Schwarcz E, Bryngelsson IL, Johannsson G. Overall and disease-specific mortality in patients with Cushing's disease: a Swedish nationwide study. J Clin Endocrinol Metab. 2019;104(6):2375–2384. doi: 10.1210/jc.2018-02524. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
