

Ethnicity influences phenotype and clinical outcomes: Comparing a South American with a North American inflammatory bowel disease cohort
- PMID: 36086782
- PMCID: PMC10980497
- DOI: 10.1097/MD.0000000000030216
Ethnicity influences phenotype and clinical outcomes: Comparing a South American with a North American inflammatory bowel disease cohort
Abstract
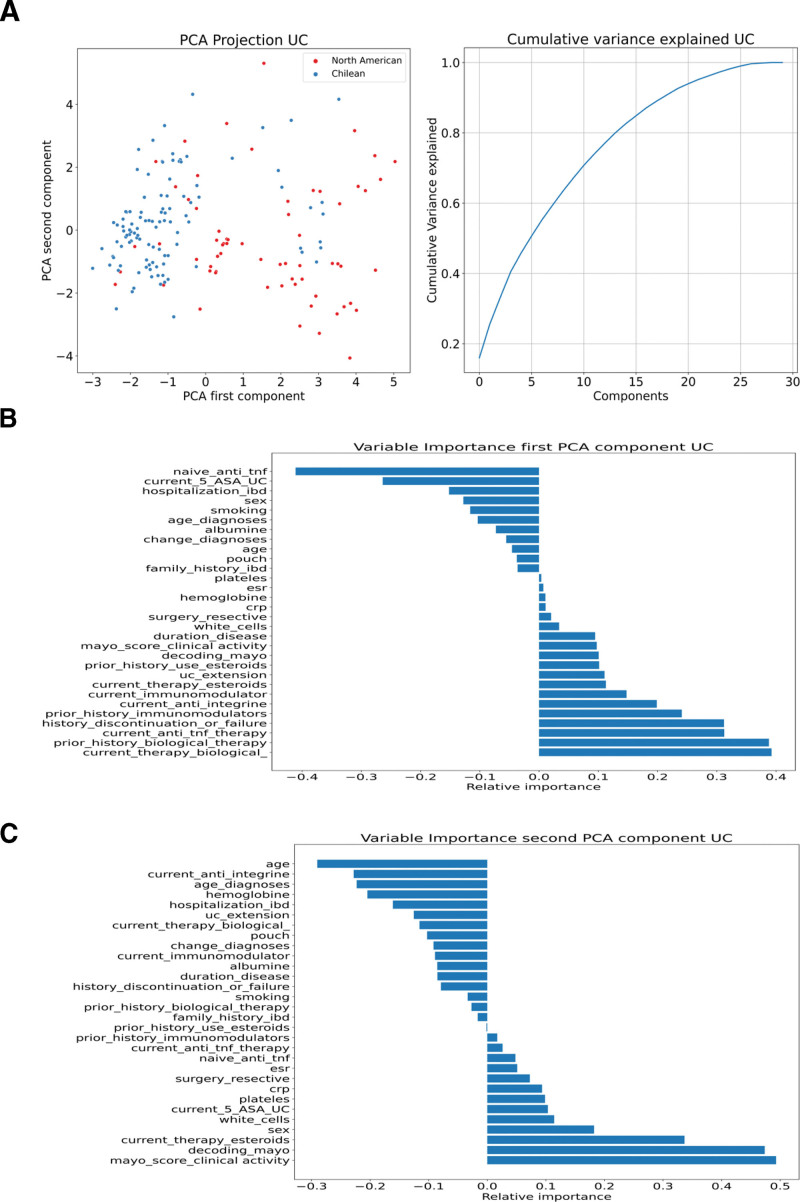
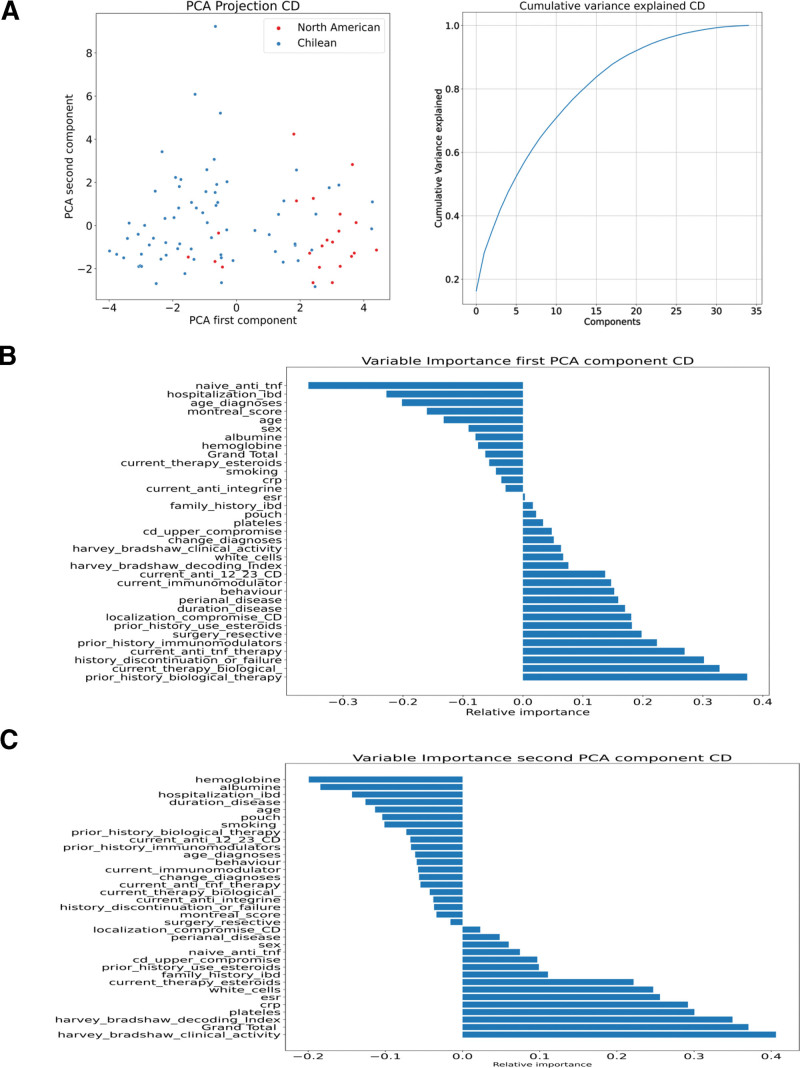
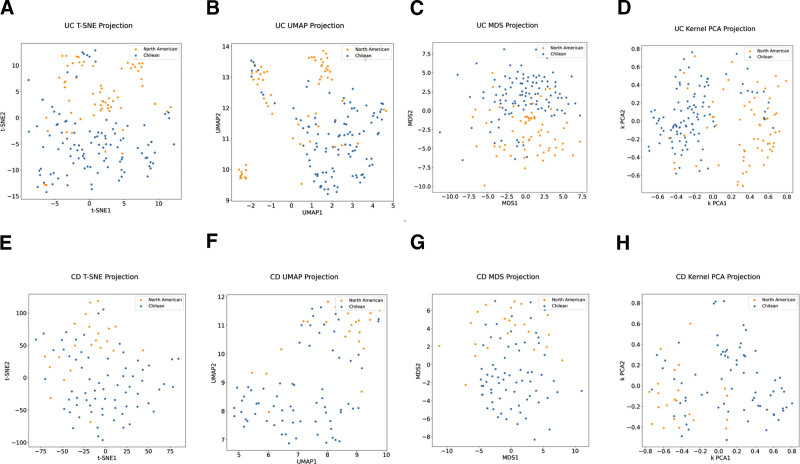
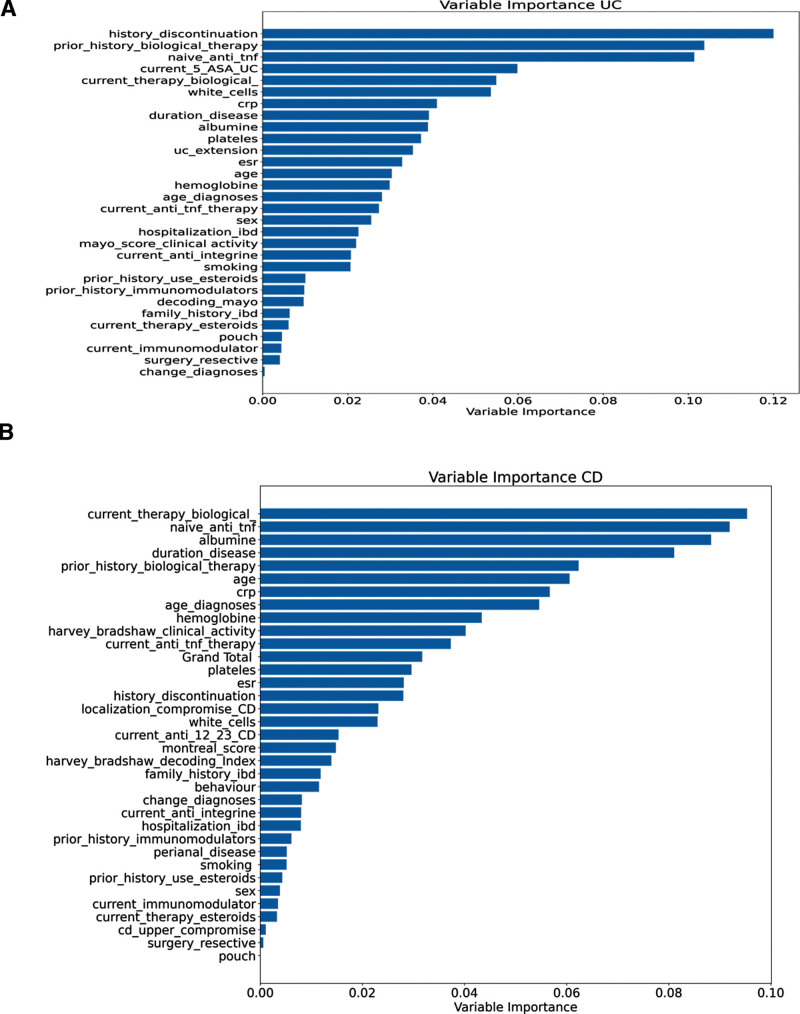
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn disease (CD), has emerged as a global disease with an increasing incidence in developing and newly industrialized regions such as South America. This global rise offers the opportunity to explore the differences and similarities in disease presentation and outcomes across different genetic backgrounds and geographic locations. Our study includes 265 IBD patients. We performed an exploratory analysis of the databases of Chilean and North American IBD patients to compare the clinical phenotypes between the cohorts. We employed an unsupervised machine-learning approach using principal component analysis, uniform manifold approximation, and projection, among others, for each disease. Finally, we predicted the cohort (North American vs Chilean) using a random forest. Several unsupervised machine learning methods have separated the 2 main groups, supporting the differences between North American and Chilean patients with each disease. The variables that explained the loadings of the clinical metadata on the principal components were related to the therapies and disease extension/location at diagnosis. Our random forest models were trained for cohort classification based on clinical characteristics, obtaining high accuracy (0.86 = UC; 0.79 = CD). Similarly, variables related to therapy and disease extension/location had a high Gini index. Similarly, univariate analysis showed a later CD age at diagnosis in Chilean IBD patients (37 vs 24; P = .005). Our study suggests a clinical difference between North American and Chilean IBD patients: later CD age at diagnosis with a predominantly less aggressive phenotype (39% vs 54% B1) and more limited disease, despite fewer biological therapies being used in Chile for both diseases.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Uhlig HH, Powrie F. Translating immunology into therapeutic concepts for inflammatory bowel disease. Annu Rev Immunol. 2018;36:755–81. - PubMed
-
- Barnes EL, Loftus EV, Jr, Kappelman MD. Effects of race and ethnicity on diagnosis and management of inflammatory bowel diseases. Gastroenterology. 2021;160:677–89. - PubMed
-
- Denson LA, Curran M, McGovern DPB, et al. Challenges in IBD research: precision medicine. Inflamm Bowel Dis. 2019;25(suppl 2):S31–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
