

Case Reports
doi: 10.1016/j.chest.2022.03.052.
A Man With Malaise, Myalgia, and Rapidly Progressive Interstitial Lung Disease
Affiliations
- PMID: 36088095
- PMCID: PMC9449304
- DOI: 10.1016/j.chest.2022.03.052
Item in Clipboard
Case Reports
A Man With Malaise, Myalgia, and Rapidly Progressive Interstitial Lung Disease
Chest.
2022 Sep.
Abstract
A 45-year-old man sought treatment at the ED during the third wave of the COVID-19 pandemic with a month-long history of fatigue, cough, myalgia, and hand stiffness. He did not report dyspnea. He had no past medical history and previously was fit and active, working as a farmer. He was a lifelong nonsmoker and had no family history of lung disease.
Copyright © 2022 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
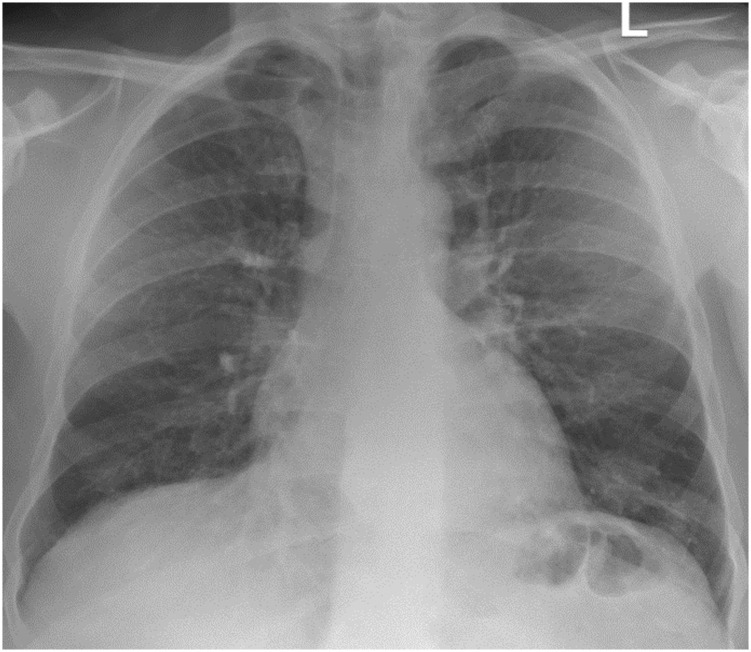
Posterior anterior chest radiograph demonstrating diffuse alveolar infiltrates bilaterally.
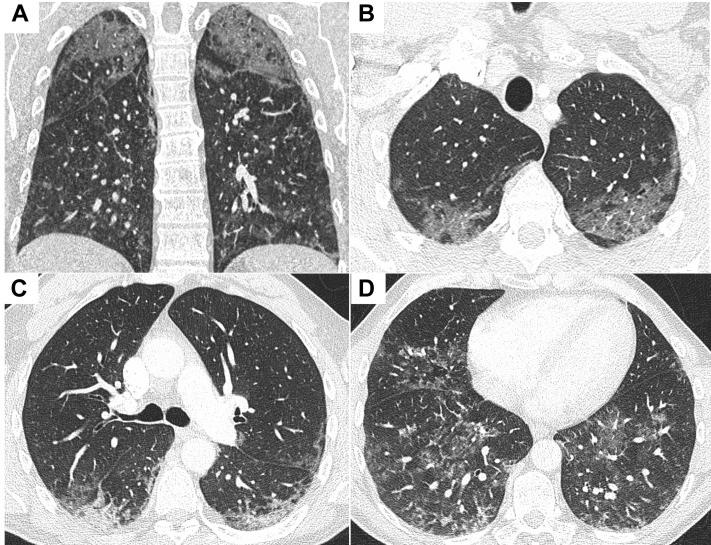
A-D, CT pulmonary angiograms demonstrating diffuse bilateral ground-glass change with reticular nodular opacities opacification in the lower lobes: coronal image (A) and axial slices from lung apices to bases (B-D).
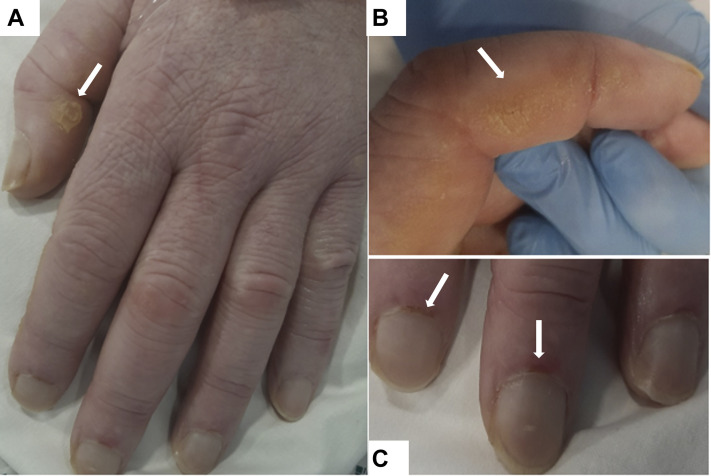
A-C, Photographs showing hyperkeratosis and skin cracking (A, B) and periungual erythema and dilated nail-fold capillaries (C).

A-C, Axial slices from a chest CT scan demonstrating progression of bilateral lower lobe consolidation and bilateral pneumothoraces with extensive subcutaneous emphysema throughout the superficial soft tissues of the chest extending into the mediastinum.
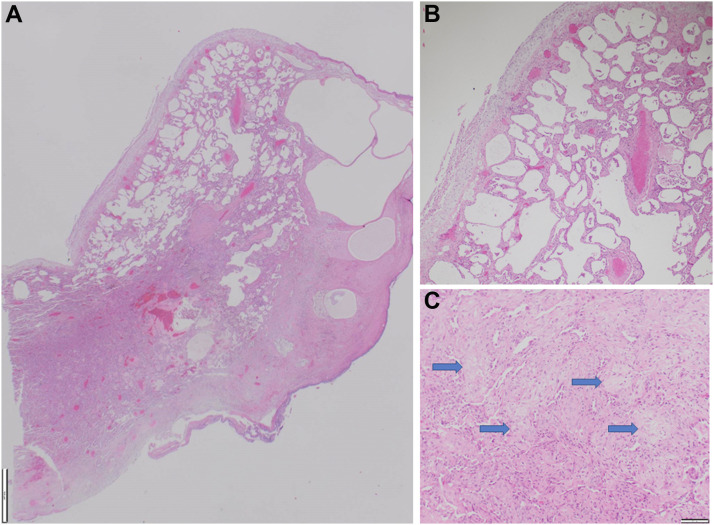
A-C, Photomicrographs of video-assisted thoracoscopic surgery lung biopsy samples showing: (A) cystically dilated subpleural alveoli and rigid-appearing alveolar walls (×125 magnification; scale bar, 1,000 μm), (B) diffuse regular interstitial expansion of alveolar walls by fibrosis consistent with a nonspecific interstitial pneumonia pattern (×100 magnification; scale bar, 100 μm), and (C) focal organizing pneumonia with endoalveolar buds (blue arrows) also present (×100 magnification; scale bar, 100 μm).
References
-
- Sato S., Hirakata M., Kuwana M., et al. Autoantibodies to a 140-kd polypeptide, CADM-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis Rheum. 2005;52(5):1571–1576. - PubMed
-
- Szodoray P., Hajas A., Kardos L., et al. Distinct phenotypes in mixed connective tissue disease: subgroups and survival. Lupus. 2012;21:1412–1422. - PubMed
-
- Sato S., Kuwana M., Fujita T., Suzuki Y. Anti-CADM-140/MDA5 autoantibody titer correlates with disease activity and predicts disease outcome in patients with dermatomyositis and rapidly progressive interstitial lung disease. Mod Rheumatol. 2013;23(3):496–502. - PubMed
-
- Ceribelli A., Fredi M., Taraborelli M., et al. Prevalence and clinical significance of anti-MDA5 antibodies in European patients with polymyositis/dermatomyositis. Clin Exp Rheumatol. 2014;32(6):891–897. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
