

Prognostic risk score development to predict birth asphyxia using maternal and fetal characteristics in South Gondar zone hospitals, north West Ethiopia
- PMID: 36088319
- PMCID: PMC9463805
- DOI: 10.1186/s12887-022-03582-x
Prognostic risk score development to predict birth asphyxia using maternal and fetal characteristics in South Gondar zone hospitals, north West Ethiopia
Abstract
Background: Birth asphyxia leads to profound systemic and neurological sequela to decrease blood flow or oxygen to the fetus followed by lethal progressive or irreversible life-long pathologies. In low resource setting countries, birth asphyxia remains a critical condition. This study aimed to develop and validate prognostic risk scores to forecast birth asphyxia using maternal and neonatal characteristics in south Gondar zone hospitals.
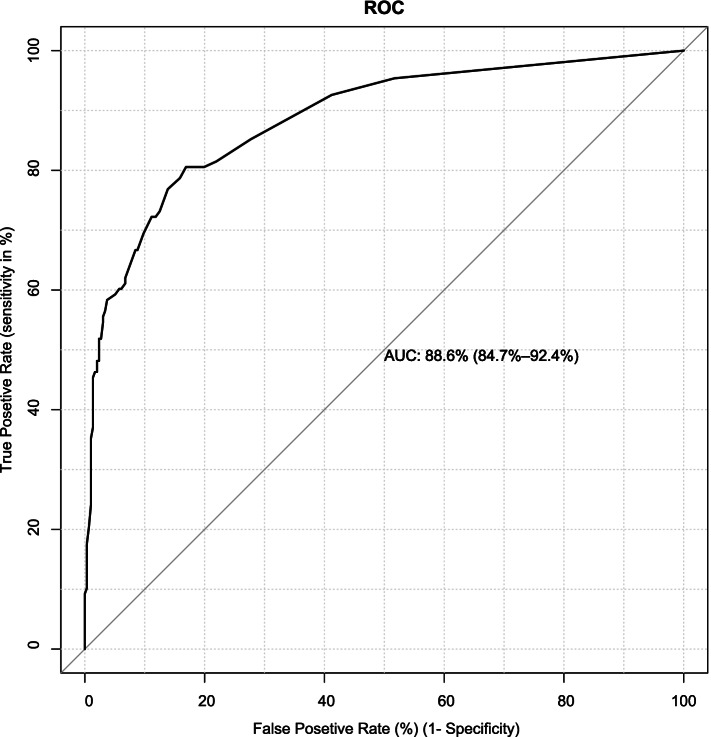
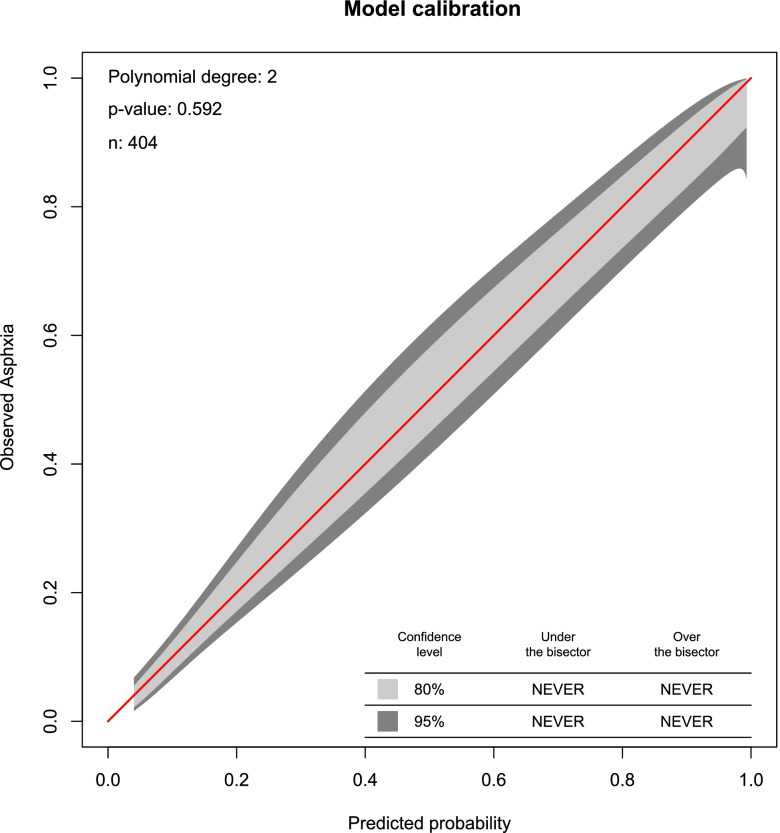
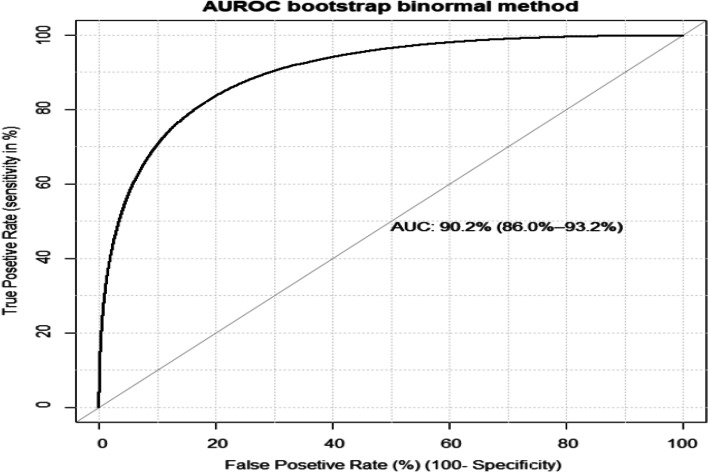
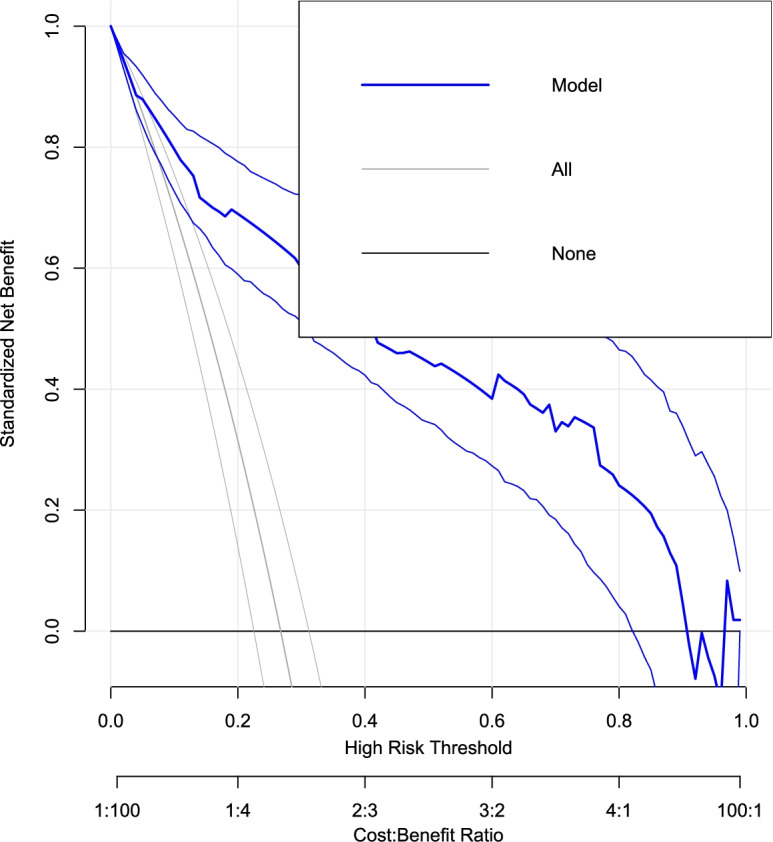
Methods: Prospective cohorts of 404 pregnant women were included in the model in south Gondar Zone Hospitals, Northwest Ethiopia. To recognize potential prognostic determinants for birth asphyxia, multivariable logistic regression was applied. The model discrimination probability was checked using the receiver operating characteristic curve (AUROC) and the model calibration plot was assessed using the 'givitiR' R-package. To check the clinical importance of the model, a cost-benefit analysis was done through a decision curve and the model was internally validated using bootstrapping. Lastly, a risk score prediction measurement was established for simple application.
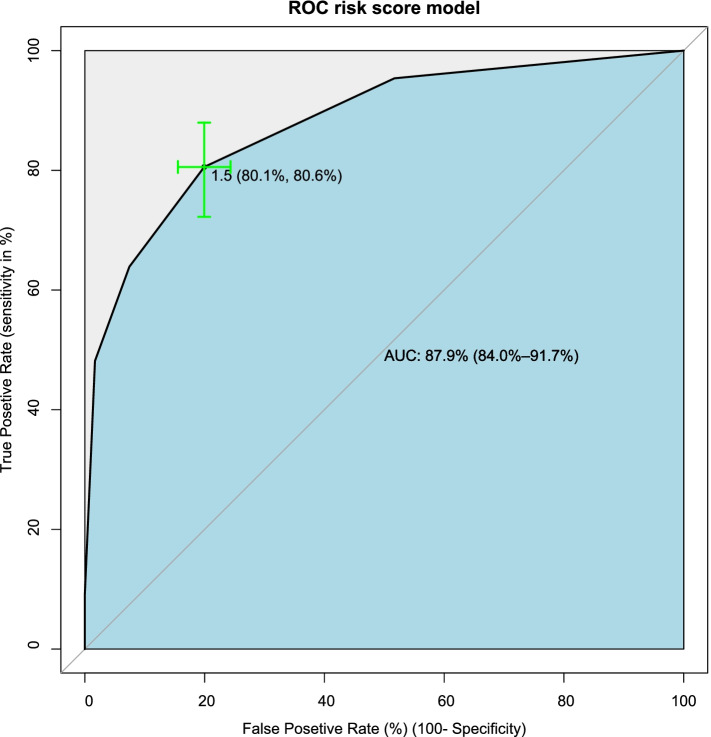
Results: Of 404, 108 (26.73%) (95% CI: 22.6-31.3) newborns were exposed to birth asphyxia during the follow-up time. Premature rupture of membrane, meconium aspiration syndrome, malpresentation, prolonged labor, Preterm, and tight nuchal was the significant prognostic predictors of birth asphyxia. The AUROC curve for birth asphyxia was 88.6% (95% CI: 84.6-92.2%), which indicated that the tool identified the newborns at risk for birth asphyxia very well. The AUROC of the simplified risk score algorithm, was 87.9 (95% CI, 84.0- 91.7%) and the risk score value of 2 was selected as the optimal cut-off value, with a sensitivity of 78.87%, a specificity of 83.26%, a positive predictive value of 63.23%, and a negative predictive value of 91.52%.
Conclusions: We established birth asphyxia prediction tools by applying non-sophisticated maternal and neonatal characteristics for resource scares countries. The driven score has very good discriminative ability and prediction performance. This risk score tool would allow reducing neonatal morbidity and mortality related to birth asphyxia. Consequently, it will improve the overall neonatal health / under-five child health in low-income countries.
Keywords: Birth asphyxia; Decision curve; Prediction; Prognostic risk score.
© 2022. The Author(s).
Conflict of interest statement
We declare that there is no competing interest with anyone else.
Figures
References
-
- Maternal and newborn health/safe motherhood unit . Division of reproductive health (technical support). Basic newborn resuscitation: a practical guide. Geneva: World Health Organization; 1997.
-
- Birth Asphyxia - Summary of the previous meeting and protocol overview. WHO Geneva Milano, 11June, 2007 .Accessed 5 Mar 2019.
-
- Keenan WJ, Udaeta E, Lopez M. Delivery and immediate neonatal care. In: Berman S, editor. Pediatric education in disasters manual. Buenos Aires: American Academy of Pediatrics; 2009. pp. 217–237.
-
- Cunningham FG, Bloom SL, Hauth JC, Rouse DJ, Spong CY, et al. Williams obstetrics. 23. USA: McGraw-Hill; 2010.
-
- WHO . Maternal and child epidemiology estimation group (MCEE). Estimates for child causes of death. 2018. pp. 2000–2016.
MeSH terms
LinkOut - more resources
Full Text Sources
