

Defining the relationship between pain intensity and disease activity in patients with rheumatoid arthritis: a secondary analysis of six studies
- PMID: 36088424
- PMCID: PMC9463789
- DOI: 10.1186/s13075-022-02903-w
Defining the relationship between pain intensity and disease activity in patients with rheumatoid arthritis: a secondary analysis of six studies
Abstract
Background: Pain is the main concern of patients with rheumatoid arthritis (RA) while reducing disease activity dominates specialist management. Disease activity assessments like the disease activity score for 28 joints with the erythrocyte sedimentation rate (DAS28-ESR) omit pain creating an apparent paradox between patients' concerns and specialists' treatment goals. We evaluated the relationship of pain intensity and disease activity in RA with three aims: defining associations between pain intensity and disease activity and its components, evaluating discordance between pain intensity and disease activity, and assessing temporal changes in pain intensity and disease activity.
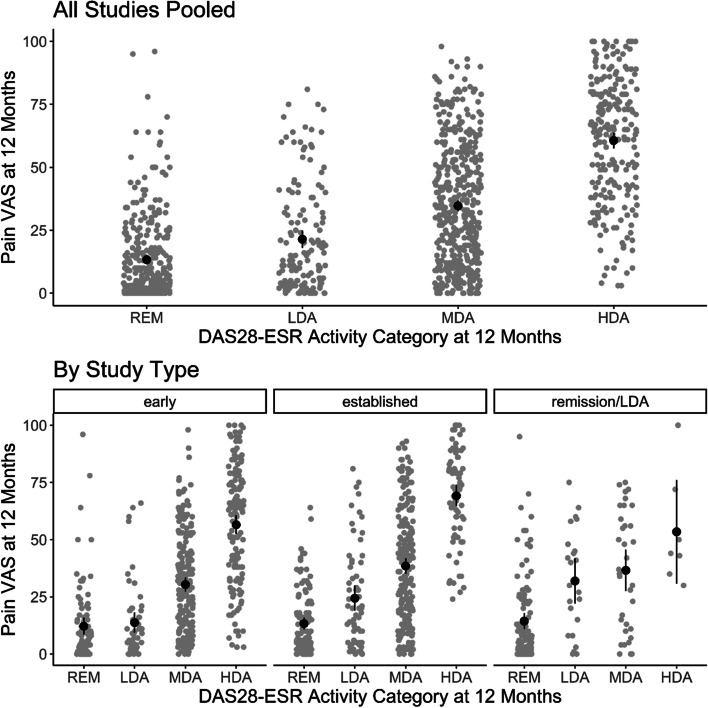
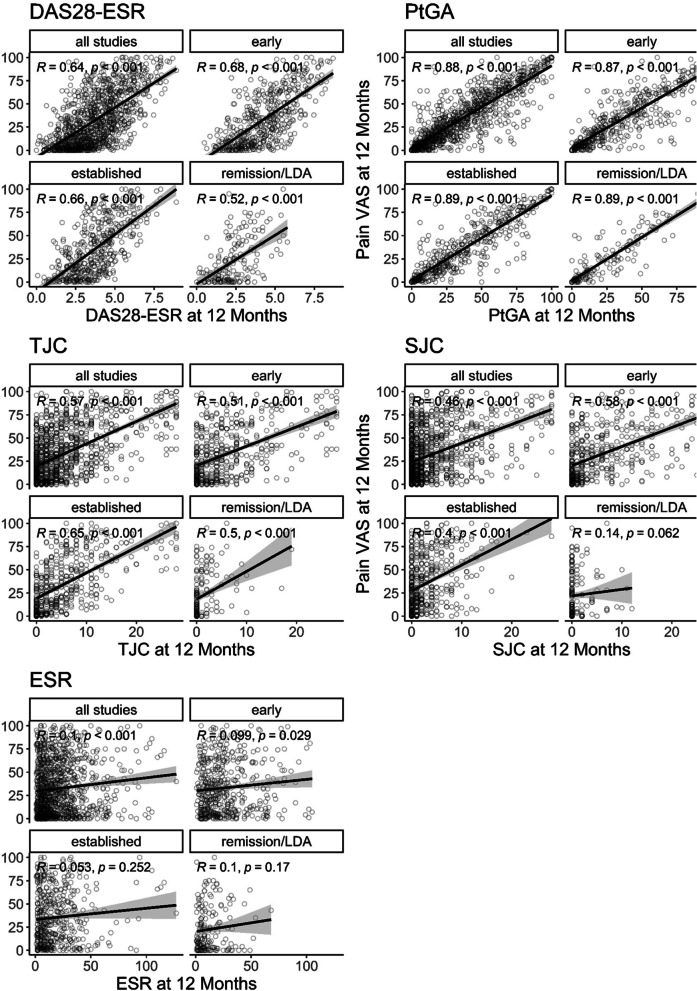
Methods: We undertook secondary analyses of five trials and one observational study of RA patients followed for 12 months. The patients had early and established active disease or sustained low disease activity or remission. Pain was measured using 100-mm visual analogue scales. Individual patient data was pooled across all studies and by types of patients (early active, established active and established remission). Associations of pain intensity and disease activity were evaluated by correlations (Spearman's), linear regression methods and Bland-Altman plots. Discordance was assessed by Kappa statistics (for patients grouped into high and low pain intensity and disease activity). Temporal changes were assessed 6 monthly in different patient groups.
Results: A total of 1132 patients were studied: 490 had early active RA, 469 had established active RA and 173 were in remission/low disease activity. Our analyses showed, firstly, that pain intensity is associated with disease activity in general, and particularly with patient global assessments, across all patient groups. Patient global assessments were a reasonable proxy for pain intensity. Secondly, there was some discordance between pain intensity and disease activity across all disease activity levels, reflecting similar discrepancies in patient global assessments. Thirdly, there were strong temporal relationships between changes in disease activity and pain intensity. When mean disease activity fell, mean pain intensity scores also fell; when mean disease activity increased, there were comparable increases in pain intensity.
Conclusions: These findings show pain intensity is an integral part of disease activity, though it is not measured directly in DAS28-ESR. Reducing disease activity is crucial for reducing pain intensity in RA.
Keywords: Disease activity assessment; Pain intensity; Remission; Rheumatoid arthritis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Smolen JS, Landewé RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, McInnes IB, Sepriano A, van Vollenhoven RF, de Wit M, Aletaha D, Aringer M, Askling J, Balsa A, Boers M, den Broeder AA, Buch MH, Buttgereit F, Caporali R, Cardiel MH, De Cock D, Codreanu C, Cutolo M, Edwards CJ, van Eijk-Hustings Y, Emery P, Finckh A, Gossec L, Gottenberg JE, Hetland ML, Huizinga TWJ, Koloumas M, Li Z, Mariette X, Müller-Ladner U, Mysler EF, da Silva JAP, Poór G, Pope JE, Rubbert-Roth A, Ruyssen-Witrand A, Saag KG, Strangfeld A, Takeuchi T, Voshaar M, Westhovens R, van der Heijde D. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79:685–699. doi: 10.1136/annrheumdis-2019-216655. - DOI - PubMed
-
- Geenen R, Overman CL, Christensen R, Åsenlöf P, Capela S, Huisinga KL, Husebø MEP, Köke AJA, Paskins Z, Pitsillidou IA, Savel C, Austin J, Hassett AL, Severijns G, Stoffer-Marx M, Vlaeyen JWS, Fernández-de-Las-Peñas C, Ryan SJ, Bergman S. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77:797–807. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
