

An external pilot cluster randomised controlled trial of a theory-based intervention to improve appropriate polypharmacy in older people in primary care (PolyPrime)
- PMID: 36088445
- PMCID: PMC9463515
- DOI: 10.1186/s40814-022-01161-6
An external pilot cluster randomised controlled trial of a theory-based intervention to improve appropriate polypharmacy in older people in primary care (PolyPrime)
Abstract
Background: For older populations with multimorbidity, polypharmacy (use of multiple medications) is a standard practice. PolyPrime is a theory-based intervention developed to improve appropriate polypharmacy in older people in primary care. This pilot study aims to assess the feasibility of the PolyPrime intervention in primary care in Northern Ireland (NI) and the Republic of Ireland (ROI).
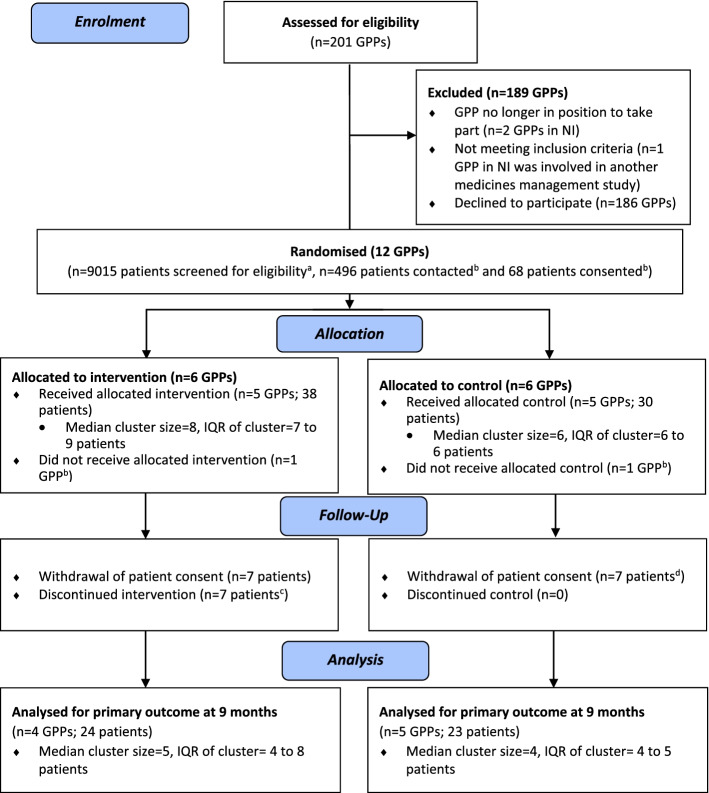
Methods: This external pilot cluster randomised controlled trial (cRCT) aimed to recruit 12 general practitioner (GP) practices (six in NI; six in the ROI counties that border NI) and ten older patients receiving polypharmacy (≥ 4 medications) per GP practice (n = 120). Practices allocated to the intervention arm watched an online video and scheduled medication reviews with patients on two occasions. We assessed the feasibility of collecting GP record (medication appropriateness, health service use) and patient self-reported data [health-related quality of life (HRQoL), health service use)] at baseline, 6 and 9 months. HRQoL was measured using the EuroQol-5 dimension-5 level questionnaire (EQ-5D-5L) and medication-related burden quality-of-life (MRB-QoL) tool. An embedded process evaluation and health economics analysis were also undertaken. Pre-specified progression criteria were used to determine whether to proceed to a definitive cRCT.
Results: Twelve GP practices were recruited and randomised. Three GP practices withdrew from the study due to COVID-related factors. Sixty-eight patients were recruited, with 47 (69.1%) being retained until the end of the study. GP record data were available for 47 patients for medication appropriateness analysis at 9 months. EQ-5D-5L and MRB-QoL data were available for 46 and 41 patients, respectively, at 9 months. GP record and patient self-reported health service use data were available for 47 patients at 9 months. Health service use was comparable in terms of overall cost estimated from GP record versus patient self-reported data. The intervention was successfully delivered as intended; it was acceptable to GPs, practice staff, and patients; and potential mechanisms of action have been identified. All five progression criteria were met (two 'Go', three 'Amend').
Conclusion: Despite challenges faced during the COVID-19 pandemic, this study has demonstrated that it may be feasible to conduct an intervention to improve appropriate polypharmacy in older people in primary care across two healthcare jurisdictions.
Trial registration: ISRCTN, ISRCTN41009897 . Registered 19 November 2019.
Clinicaltrials: gov, NCT04181879 . Registered 02 December 2019.
Keywords: Behaviour change; Complex intervention; General practice; Older people; Pilot study; Polypharmacy; Prescribing; Primary care; Process evaluation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- McGarrigle C, Donoghue O, Scarlett S, Kenny RA. Health and wellbeing: active ageing for older adults in Ireland. Dublin: The Irish Longitudinal Study on Ageing (TILDA): 2017. https://tilda.tcd.ie/publications/reports/pdf/w3-key-findings-report/TIL.... Accessed 26 Feb 2022.
-
- World Health Organisation . Medication safety in polypharmacy. Geneva: World Health Organization; 2019.
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
