

Use of failure-to-rescue after emergency surgery as a dynamic indicator of hospital resilience during the COVID-19 pandemic. A multicenter retrospective propensity score-matched cohort study
- PMID: 36089261
- PMCID: PMC9458615
- DOI: 10.1016/j.ijsu.2022.106890
Use of failure-to-rescue after emergency surgery as a dynamic indicator of hospital resilience during the COVID-19 pandemic. A multicenter retrospective propensity score-matched cohort study
Abstract
Background: Surgical failure-to-rescue (FTR, death rate following complications) is a reliable cross-sectional quality of care marker, but has not been evaluated dynamically. We aimed to study changes in FTR following emergency surgery during the COVID-19 pandemic.
Material and methods: Matched cohort study including all COVID-19-non-infected adult patients undergoing emergency general surgery in 25 Spanish hospitals during COVID-19 pandemic peak (March-April 2020), non-peak (May-June 2020), and 2019 control periods. A propensity score-matched comparative analysis was conducted using a logistic regression model, in which period was regressed on observed baseline characteristics. Subsequently, a mixed effects logistic regression model was constructed for each variable of interest. Main variable was FTR. Secondary variables were post-operative complications, readmissions, reinterventions, and length of stay.
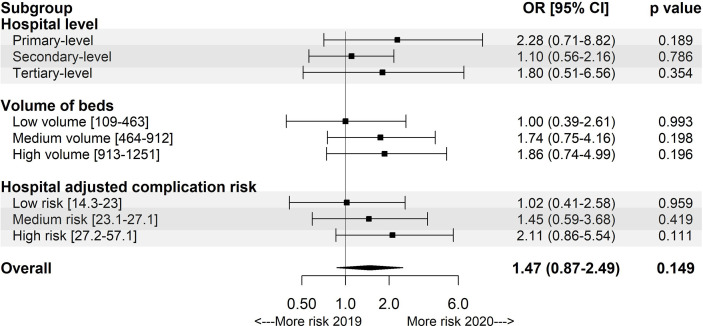
Results: 5003 patients were included (948, 1108, and 2947 in the pandemic peak, non-peak, and control periods), with comparable clinical characteristics, prognostic scores, complications, reintervention, rehospitalization rates, and length of stay across periods. FTR was greater during the pandemic peak than during non-peak and pre-pandemic periods (22.5% vs. 17.2% and 12.7%), being this difference confirmed in adjusted analysis (odds ratio [OR] 2.13, 95% confidence interval [95% CI] 1.27-3.66). There was sensible inter-hospital variability in FTR changes during the pandemic peak (median FTR change +8.77%, IQR 0-29.17%) not observed during the pandemic non-peak period (median FTR change 0%, IQR -6.01-6.72%). Greater FTR increase was associated with higher COVID-19 incidence (OR 2.31, 95% CI 1.31-4.16) and some hospital characteristics, including tertiary level (OR 3.07, 95% CI 1.27-8.00), medium-volume (OR 2.79, 95% CI 1.14-7.34), and high basal-adjusted complication risk (OR 2.21, 95% CI 1.07-4.72).
Conclusion: FTR following emergency surgery experienced a heterogeneous increase during different periods of the COVID-19 pandemic, suggesting it to behave as an indicator of hospital resilience. FTR monitoring could facilitate identification of centres in special needs during ongoing health care challenges.
Keywords: COVID-19; Emergency surgery; Failure-to-rescue; Resilience.
Copyright © 2022 IJS Publishing Group Ltd. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors have no competing interests to declare.
Figures


References
-
- International Strategy for Disaster Reduction . World Conference on Disaster Reduction, 18–22 January 2005. Kobe, Hyogo, Japan; 2005. Hyogo framework for action 2005–2015: building the resilience of nations and communities to disasters.https://www.unisdr.org/2005/wcdr/intergover/official-doc/L-docs/Hyogo-fr... accessed.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
