

Major haemorrhage: past, present and future
- PMID: 36089857
- PMCID: PMC10087440
- DOI: 10.1111/anae.15866
Major haemorrhage: past, present and future
Abstract
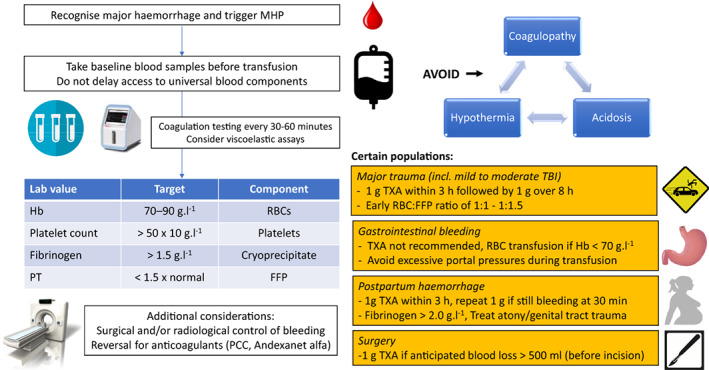
Major haemorrhage is a leading cause of morbidity and mortality worldwide. Successful treatment requires early recognition, planned responses, readily available resources (such as blood products) and rapid access to surgery or interventional radiology. Major haemorrhage is often accompanied by volume loss, haemodilution, acidaemia, hypothermia and coagulopathy (factor consumption and fibrinolysis). Management of major haemorrhage over the past decade has evolved to now deliver a 'package' of haemostatic resuscitation including: surgical or radiological control of bleeding; regular monitoring of haemostasis; advanced critical care support; and avoidance of the lethal triad of hypothermia, acidaemia and coagulopathy. Recent trial data advocate for a more personalised approach depending on the clinical scenario. Fresh frozen plasma should be given as early as possible in major trauma in a 1:1 ratio with red blood cells until the results of coagulation tests are available. Tranexamic acid is a cheap, life-saving drug and is advocated in major trauma, postpartum haemorrhage and surgery, but not in patients with gastrointestinal bleeding. Fibrinogen levels should be maintained > 2 g.l-1 in postpartum haemorrhage and > 1.5 g.l-1 in other haemorrhage. Improving outcomes after major traumatic haemorrhage is now driving research to include extending blood-product resuscitation into prehospital care.
Keywords: crystalloid resuscitation: coagulopathy; major haemorrhage; transfusion; trauma.
© 2022 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures
References
-
- Curry NS, Davenport R. Transfusion strategies for major haemorrhage in trauma. British Journal of Haematology 2019; 184: 508–23. - PubMed
-
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Global Health 2014; 2: e323–33. - PubMed
-
- Halmin M, Chiesa F, Vasan SK, et al. Epidemiology of massive transfusion: a binational study from Sweden and Denmark. Critical Care Medicine 2016; 44: 468–77. - PubMed
-
- Sperry JL, Guyette FX, Brown JB, et al. Prehospital plasma during air medical transport in trauma patients at risk for hemorrhagic shock. New England Journal of Medicine 2018; 379: 315–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
