

Association of Parasomnia Symptoms with Risk of Childhood Asthma and the Role of Preterm Birth
- PMID: 36089999
- PMCID: PMC9451036
- DOI: 10.2147/NSS.S356182
Association of Parasomnia Symptoms with Risk of Childhood Asthma and the Role of Preterm Birth
Abstract
Purpose: To examine whether parasomnia symptoms are associated with increased odds of childhood asthma and wheeze, and the role of preterm birth.
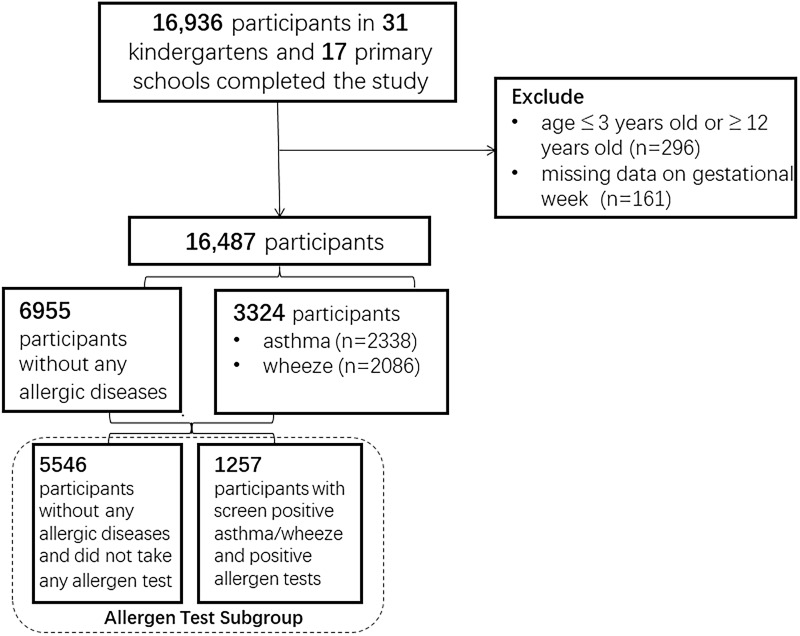
Patients and methods: The Shanghai Children's Allergy Study was cross-sectionally conducted in 31 kindergartens and 17 primary schools in Shanghai, China. After excluding the missing data of gestational week and child's age, this study included a total of 16,487 individuals with a mean age of 7.74 years and 52.4% of males. The association between parasomnia symptoms and wheeze/asthma was assessed by univariate and multivariate analyses. The interaction effects of parasomnias and preterm birth were primarily evaluated by P for multiplicative interaction, and the relative excess risk due to interaction (RERI), attributable proportion due to interaction (AP), and synergy index (SI) were also measured.
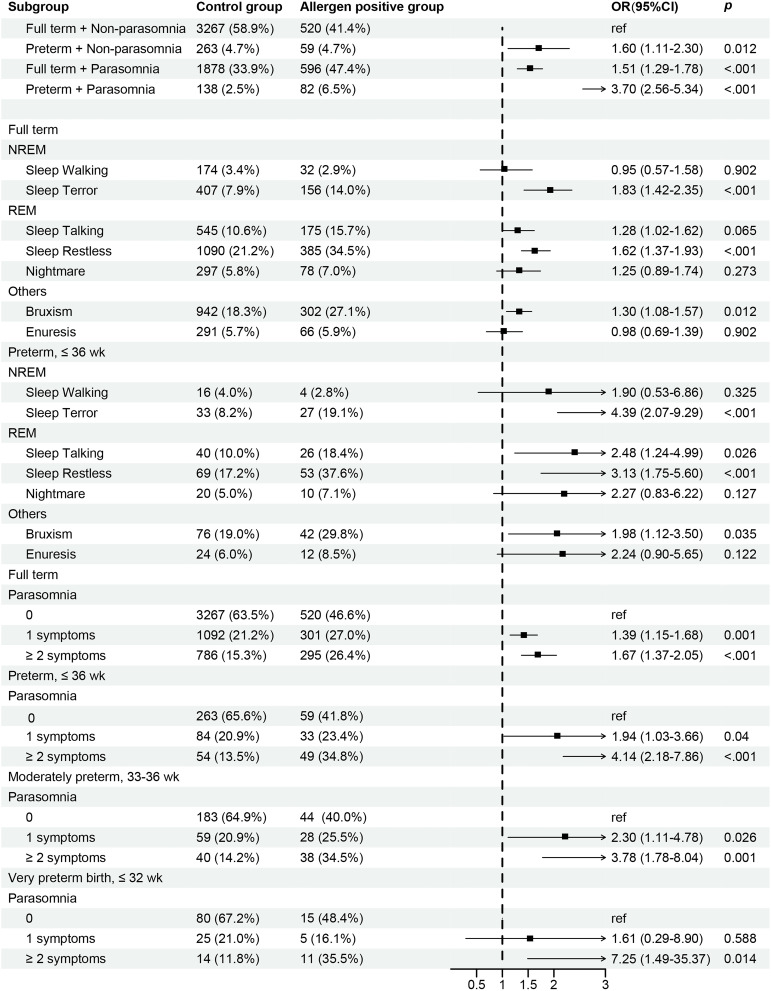
Results: Parasomnias, especially rapid eye movement (REM) parasomnia symptoms, were associated with an increased risk of childhood wheeze/asthma, and the interaction between parasomnia and preterm birth exhibited an excess risk of current wheeze (RERI, 1.43; 95% CI, 0.41-2.45) and ever asthma (RERI, 0.75; 95% CI, 0.01-1.50). In the stratification analyses, the combination of parasomnia symptoms and preterm birth had higher odds of wheeze/asthma. And the odds of current wheeze (OR, 4.55; 95% CI, 1.69-12.25; p=0.003) and ever asthma (OR, 6.17; 95% CI, 2.36-16.11; p<0.001) were much higher in cumulative parasomnia symptoms plus very preterm birth. And sensitive analyses were further conducted in populations without sleep disordered breathing (SDB), and an allergen test subgroup, yielding similar results.
Conclusion: Parasomnia symptoms are associated with increased odds of childhood wheeze/asthma, and the odds were even higher in premature population. The findings suggest that parasomnia symptoms, as a developmental sleep disorder, are supposed to be closely watched among children who have asthma or are at risk for asthma, and that preterm children deserve more attention.
Keywords: premature; respiratory allergies; sleep; sleep disorders.
© 2022 Chen et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Zadra A, Pilon M. NREM parasomnias - ScienceDirect. Handb Clin Neurol. 2011;99:851–868. - PubMed
LinkOut - more resources
Full Text Sources
