

High-level resistance to non-nucleos(t)ide reverse transcriptase inhibitor based first-line antiretroviral therapy in Ghana; A 2017 study
- PMID: 36090108
- PMCID: PMC9459847
- DOI: 10.3389/fmicb.2022.973771
High-level resistance to non-nucleos(t)ide reverse transcriptase inhibitor based first-line antiretroviral therapy in Ghana; A 2017 study
Abstract
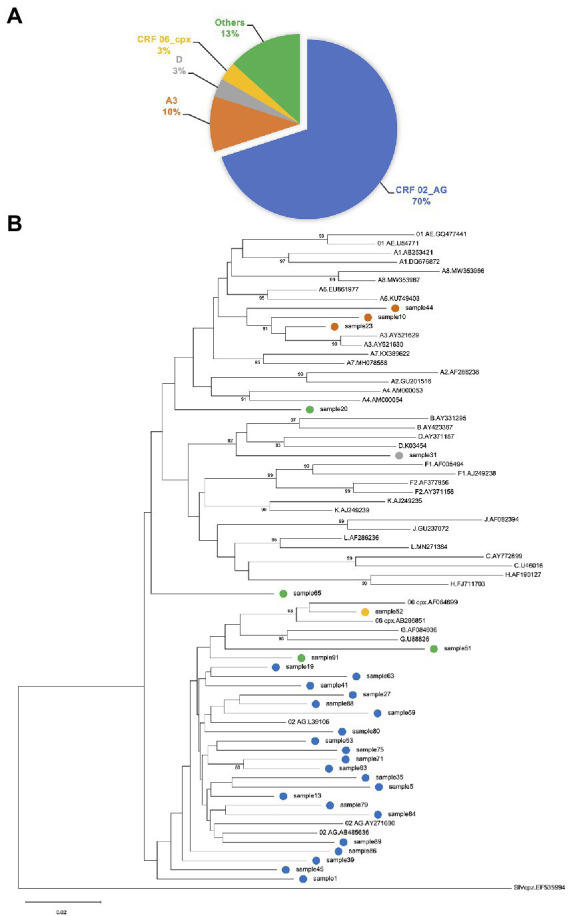
Expanding access to effective antiretroviral therapy (ART) is a major tool for management of Human Immunodeficiency Virus (HIV) infection. However, rising levels of HIV drug-resistance have significantly hampered the anticipated success of ART in persons living with HIV (PLWH), particularly those from Africa. Though great strides have been made in Ghana toward achieving the UNAIDS "95-95-95" target, a substantial number of PLWH receiving ART have not attained viral suppression. This study investigated patterns of drug resistance mutations in ART naïve as well as ART-experienced PLWH receiving first-line regimen drugs from Ghana. In a cross-sectional study, blood samples were collected from HIV-1 infected adults (≥18 years) attending HIV/AIDS clinic at the Eastern Regional Hospital, Koforidua, Ghana from September to October 2017. Viral RNA isolated from plasma were subjected to genotypic drug resistance testing for Protease Inhibitors (PI), Reverse Transcriptase Inhibitors (RTI), and Integrase Strand Transfer Inhibitors (INSTI). A total of 95 (84 ART experienced, 11 ART naïve) HIV-1 infected participants were sampled in this study. Sixty percent (50/84) of the ART-experienced participants were controlling viremia (viral load < 1,000 copies/ml). Of the 95 patient samples, 32, 34, and 33 were successfully sequenced for protease, reverse-transcriptase, and integrase regions, respectively. The dominant HIV-1 subtypes detected were CRF02_AG (70%), and A3 (10%). Major drug resistance associated mutations were only detected for reverse transcriptase inhibitors. The predominant drug resistance mutations were against nucleos(t)ide reverse transcriptase inhibitors (NRTI)-M184V/I and non-nucleos(t)ide reverse transcriptase inhibitors (NNRTI)-K103N. In the ART-experienced group, M184V/I and K103N were detected in 54% (15/28) and 46% (13/28) of individuals, respectively. Both mutations were each detected in 33% (2/6) of ART naïve individuals. Multiclass resistance to NRTI and NNRTI was detected in 57% of ART-experienced individuals and two ART naïve individuals. This study reports high-level resistance to NNRTI-based antiretroviral therapy in PLWH in Ghana. However, the absence of major PI and INSTI associated-mutations is a good signal that the current WHO recommendation of Dolutegravir in combination with an NRTI backbone will yield maximum benefits as first-line regimen for PLWH in Ghana.
Keywords: Ghana; HIV-1; drug resistance; integrase strand transfer inhibitors; non-nucleos(t)ide reverse transcriptase inhibitors; nucleos(t)ide reverse transcriptase inhibitors; protease inhibitors.
Copyright © 2022 Parbie, Abana, Kushitor, Asigbee, Ntim, Addo-Tetebo, Ansong, Ofori, Mizutani, Runtuwene, Nishizawa, Ishikawa, Kiyono, Ampofo, Matano, Bonney and Kikuchi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Aghokeng A. F., Kouanfack C., Laurent C., Ebong E., Atem-Tambe A., Butel C., et al. (2011). Scale-up of antiretroviral treatment in sub-Saharan Africa is accompanied by increasing HIV-1 drug resistance mutations in drug-naive patients. AIDS 25, 2183–2188. doi: 10.1097/QAD.0b013e32834bbbe9, PMID: - DOI - PubMed
-
- ANRS (2015). ANRS AC11 resistance study group PCR and sequencing procedures: HIV-1. Version January 2015. Available at: https://hivfrenchresistance.org/wp-content/uploads/2021/10/ANRS-procedur... (Accessed July 5, 2022).
-
- ANRS (2021). HIV-1 Genotypic Drug Resistance Interpretation Algorithm. Available at: https://hivfrenchresistance.org/hiv-french-resitance-tables-of-rules (Accessed February 1, 2022).
-
- Deletsu S. D., Maina E. K., Quaye O., Ampofo W. K., Awandare G. A., Bonney E. Y. (2020). High resistance to reverse transcriptase inhibitors among persons infected with human immunodeficiency virus type 1 subtype circulating recombinant form 02_AG in Ghana and on antiretroviral therapy. Medicine 99:e18777. doi: 10.1097/MD.0000000000018777, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous