

Independent predictors and risk score for intraprocedural rupture during endovascular treatment of small ruptured intracranial aneurysms (<5 mm)
- PMID: 36090846
- PMCID: PMC9449369
- DOI: 10.3389/fneur.2022.923645
Independent predictors and risk score for intraprocedural rupture during endovascular treatment of small ruptured intracranial aneurysms (<5 mm)
Abstract
Background and purpose: Intraprocedural rupture (IPR) is a devastating complication of endovascular treatment (EVT). Small-sized and ruptured aneurysms are independent predictors of IPR, which presents a technical challenge during EVT. We aimed to develop a score to quantify the individual patient risk of IPR in the EVT of small (<5 mm) ruptured aneurysms (SRAs).
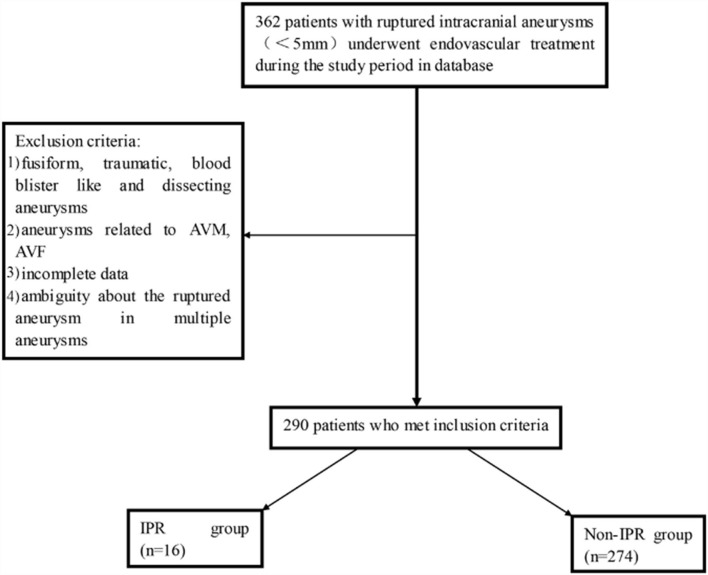
Methods: A retrospective review was conducted to interrogate databases prospectively maintained at two academic institutions in China from January 2009 to October 2016. We collected intraoperative angiograms and medical records to identify independent predictors of IPR using univariate and multivariable analyses. A risk score for IPR was derived using multivariable logistic regression analyses.
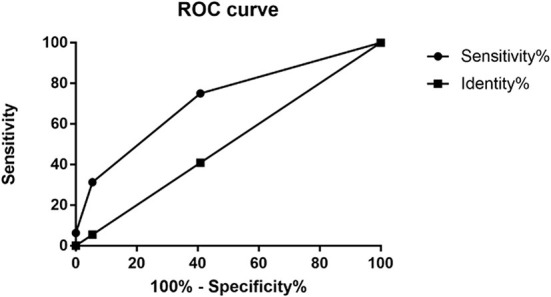
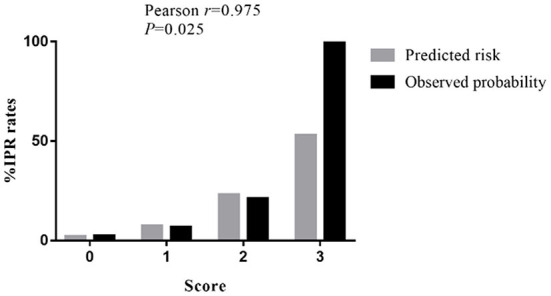
Results: Of the 290 enrolled patients, IPR occurred in 16 patients (5.5%). The univariate analysis showed that the rate of IPR was significantly higher in patients having aneurysms with a small basal outpouching (SBO), in patients having aneurysms concomitant with adjacent moderate atherosclerotic stenosis (ACAMAS), and in former or current smokers. Multivariate analyses showed that SBO [odds ratio (OR): 3.573; 95% confidence interval (CI): 1.078-11.840; p = 0.037], vascular eloquence (VE; OR: 3.780; 95% CI: 1.080-13.224; p = 0.037), and ACAMAS (OR: 6.086; 95% CI: 1.768-20.955; p = 0.004) were significantly and independently associated with IPR. A three-point risk score (S-V-A) was derived to predict IPR [SBO (yes = 1), VE (yes = 1), and ACAMAS (yes = 1)].
Conclusions: Intraprocedural rupture occurred in 5.5% of the patients during EVT of SRA. SBO, VE, and ACAMAS were independent risk factors of IPR in the EVT of SRA. Based on these variables, the S-V-A score may be useful in predicting IPR daily, but more confirmation studies are required.
Keywords: endovascular treatment; intracranial aneurysms; intraprocedural rupture; risk score; small.
Copyright © 2022 Peng, Feng, He, Niu, Zhang, Tong, Zhang, Xia, Chen, Xu, Qi, Lu, Wang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Anokwute MC, Braca JA, Bohnstedt B, DeNardo A, Scott J, Cohen-Gadol A, et al. Endovascular treatment of ruptured tiny (≤ 3 mm) intracranial aneurysms in the setting of subarachnoid hemorrhage: a case series of 20 patients and literature review. J Clin Neurosci. (2017) 40:52–6. 10.1016/j.jocn.2017.01.011 - DOI - PubMed
LinkOut - more resources
Full Text Sources