

Transtibial Pullout Repair of Lateral Meniscus Posterior Root Tear with Tissue Loss: A Case with Anterior Cruciate Ligament Injury and Medial Meniscus Tear
- PMID: 36092283
- PMCID: PMC9453023
- DOI: 10.1155/2022/9776388
Transtibial Pullout Repair of Lateral Meniscus Posterior Root Tear with Tissue Loss: A Case with Anterior Cruciate Ligament Injury and Medial Meniscus Tear
Abstract
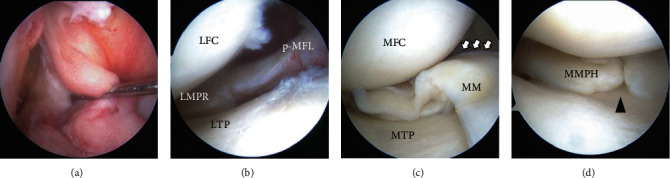
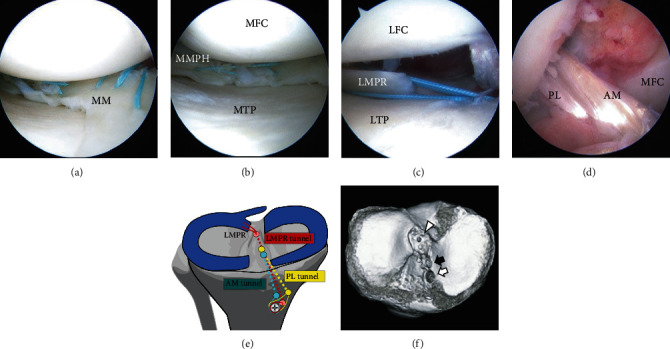
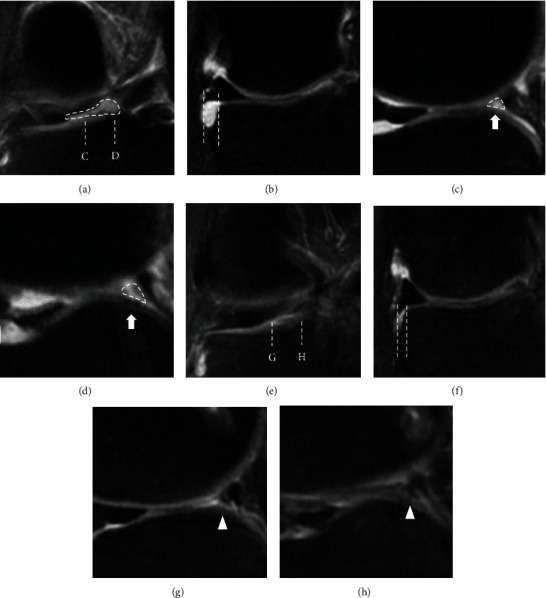
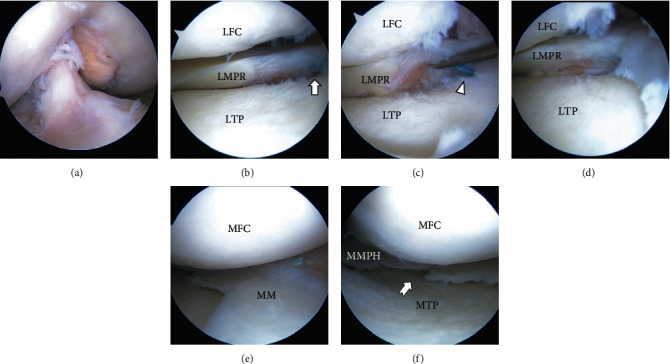
Lateral meniscus (LM) posterior root tear (LMPRT) is mainly caused by trauma, especially trauma associated with anterior cruciate ligament (ACL) injuries. Although a transtibial pullout repair or a side-to-side repair is commonly performed for LMPRT, to the best of our knowledge, there is no clinical report of LMPRT with tissue loss using the pullout technique. Thus, the purpose of this report was to describe a clinical, radiographic, and arthroscopic outcome after pullout repair for a case of LMPRT with a large defect with a chronic ACL tear and complex medial meniscus (MM) tears. A 31-year-old man complained of knee pain and restricted range of motion after twisting his knee when he stepped on an iron pipe. The patient had a football-related injury to his right knee 14 years before presentation, and since then, the patient's knee has given out more than 10 times but was left unassessed. Magnetic resonance imaging showed LMPRT with tissue loss, ACL tears, and complex MM tears. Transtibial pullout repair of the LMPRT with ACL reconstruction and MM repairs were performed. Following the pullout repair of the LMPRT, an approximately 6 mm gap remained between the LM posterior root and root insertion. However, magnetic resonance imaging and second-look arthroscopy at 1 year postoperatively revealed meniscal healing, gap filling with some regeneration tissue, of the LM posterior root. Furthermore, the lateral meniscus extrusion in the coronal plane improved from 3.1 mm (preoperative) to 1.6 mm (1 year postoperatively). Transtibial pullout repair with the remaining gap could be a viable treatment option for LMPRT with tissue loss, combined with ACL reconstruction.
Copyright © 2022 Masanori Tamura et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Figures
Similar articles
-
Transtibial pullout repair of the lateral meniscus posterior root tear combined with anterior cruciate ligament reconstruction reduces lateral meniscus extrusion: A retrospective study.Orthop Traumatol Surg Res. 2020 May;106(3):469-473. doi: 10.1016/j.otsr.2019.10.022. Epub 2020 Apr 8. Orthop Traumatol Surg Res. 2020. PMID: 32278734
-
Shared ACL Bone Tunnel Technique for Repair of Lateral Meniscus Posterior Root Tears Combined With ACL Reconstruction.Orthop J Sports Med. 2022 Aug 17;10(8):23259671221114319. doi: 10.1177/23259671221114319. eCollection 2022 Aug. Orthop J Sports Med. 2022. PMID: 36003966 Free PMC article.
-
Complete tear of the lateral meniscus posterior root is associated with meniscal extrusion in anterior cruciate ligament deficient knees.J Orthop Res. 2018 Jul;36(7):1894-1900. doi: 10.1002/jor.23861. Epub 2018 Feb 21. J Orthop Res. 2018. PMID: 29369416
-
A narrative review of lateral meniscus root tears and extrusion: techniques and outcomes.Ann Jt. 2022 Apr 15;7:15. doi: 10.21037/aoj-20-112. eCollection 2022. Ann Jt. 2022. PMID: 38529138 Free PMC article. Review.
-
Arthroscopic meniscal repair with use of the outside-in technique.Instr Course Lect. 2000;49:195-206. Instr Course Lect. 2000. PMID: 10829175 Review.
Cited by
-
Diagnosis and Treatment Strategies of Meniscus Root Tears: A Scoping Review.Orthop J Sports Med. 2024 Nov 1;12(11):23259671241283962. doi: 10.1177/23259671241283962. eCollection 2024 Nov. Orthop J Sports Med. 2024. PMID: 39493310 Free PMC article.
References
-
- Praz C., Vieira T. D., Saithna A., et al. Risk factors for lateral meniscus posterior root tears in the anterior cruciate ligament-injured knee: an epidemiological analysis of 3956 patients from the SANTI Study Group. The American Journal of Sports Medicine . 2019;47(3):598–605. doi: 10.1177/0363546518818820. - DOI - PubMed
-
- Minami T., Muneta T., Sekiya I., et al. Lateral meniscus posterior root tear contributes to anterolateral rotational instability and meniscus extrusion in anterior cruciate ligament-injured patients. Knee Surgery, Sports Traumatology, Arthroscopy . 2017;26(4):1174–1181. doi: 10.1007/s00167-017-4569-8. - DOI - PubMed
-
- Frank J. M., Moatshe G., Brady A. W., et al. Lateral meniscus posterior root and meniscofemoral ligaments as stabilizing structures in the acl-deficient knee: a biomechanical study. Orthopaedic Journal of Sports Medicine . 2017;5(6, article 2325967117695756) doi: 10.1177/2325967117695756. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
