

Therapeutic Lumbar Punctures in Human Immunodeficiency Virus-Associated Cryptococcal Meningitis: Should Opening Pressure Direct Management?
- PMID: 36092828
- PMCID: PMC9454029
- DOI: 10.1093/ofid/ofac416
Therapeutic Lumbar Punctures in Human Immunodeficiency Virus-Associated Cryptococcal Meningitis: Should Opening Pressure Direct Management?
Abstract
Background: Increased intracranial pressure (ICP) frequently complicates cryptococcal meningitis. Therapeutic lumbar punctures (LPs) have acute survival benefits in the first week, and we sought to understand the longer-term survival impact of therapeutic LPs.
Methods: We prospectively enrolled human immunodeficiency virus (HIV)-seropositive adults with cryptococcal meningitis from 2013 to 2017 in Uganda. We assessed the association between clinical characteristics, CSF parameters, and 14- and 30-day mortality by baseline ICP. We also assessed 30-day mortality by number of follow-up therapeutic LPs performed within 7 days.
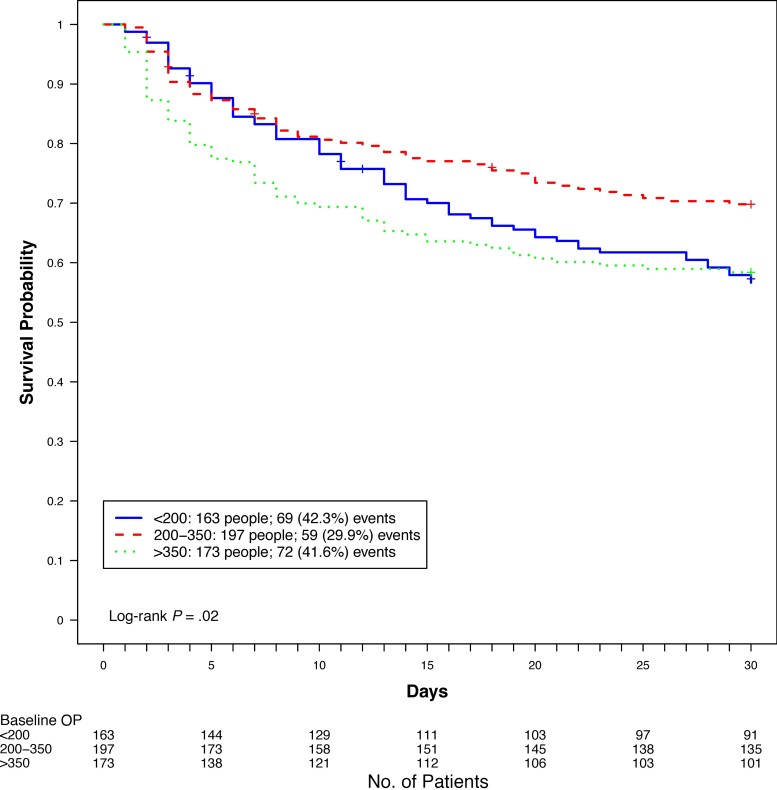
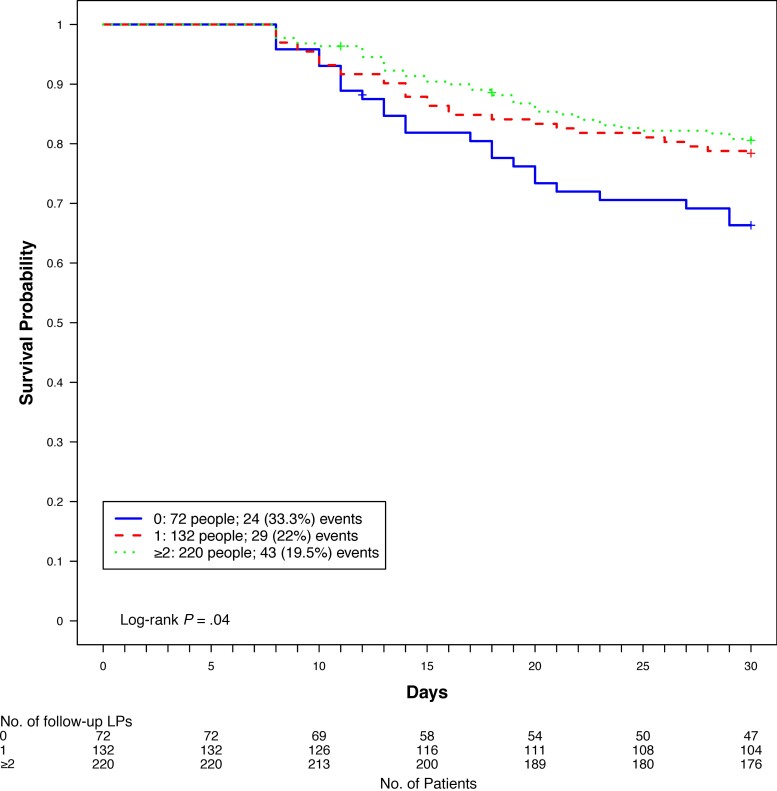
Results: Our analysis included 533 participants. Participants with baseline ICP >350 mm H2O were more likely to have Glasgow Coma Scale (GCS) score <15 (P < .001), seizures (P < .01), and higher quantitative cryptococcal cultures (P < .001), whereas participants with ICP <200 mm H2O were more likely to have baseline sterile CSF cultures (P < .001) and CSF white blood cell count ≥5 cells/µL (P = .02). Thirty-day mortality was higher in participants with baseline ICP >350 mm H2O and ICP <200 mm H2O as compared with baseline ICP 200-350 mm H2O (hazard ratio, 1.55 [95% confidence interval, 1.10-2.19]; P = .02). Among survivors at least 7 days, the 30-day relative mortality was 50% higher among participants who did not receive any additional therapeutic LPs compared to those with ≥1 additional follow-up LP (33% vs 22%; P = .04), irrespective of baseline ICP.
Conclusions: Management of increased ICP remains crucial in improving clinical outcomes in cryptococcal meningitis. Guidelines should consider an approach to therapeutic LPs that is not dictated by baseline ICP.
Keywords: baseline opening pressure; cryptococcal meningitis; mortality; therapeutic lumbar puncture.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Diamond RD, Bennett JE. Prognostic factors in cryptococcal meningitis. A study in 111 cases. Ann Intern Med 1974; 80:176–81. - PubMed
-
- Denning DW, Armstrong RW, Lewis BH, Stevens DA. Elevated cerebrospinal fluid pressures in patients with cryptococcal meningitis and acquired immunodeficiency syndrome. Am J Med 1991; 91:267–72. - PubMed
