

Extracranial metastasis of glioblastoma with genomic analysis: a case report and review of the literature
- PMID: 36093544
- PMCID: PMC9459505
- DOI: 10.21037/tcr-22-955
Extracranial metastasis of glioblastoma with genomic analysis: a case report and review of the literature
Abstract
Background: Glioblastoma (GBM) is the first most frequent type of primary malignant brain tumors in adults. It is basically confined to the brain, and extracranial metastases (ECM) are rare. The genomic features of GBM with ECM are not fully elucidated.
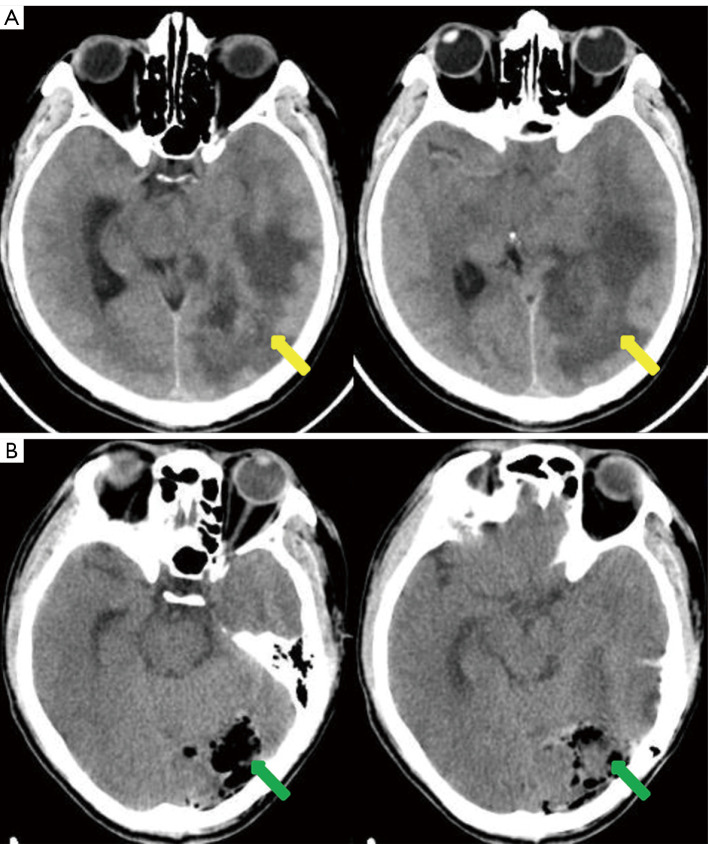
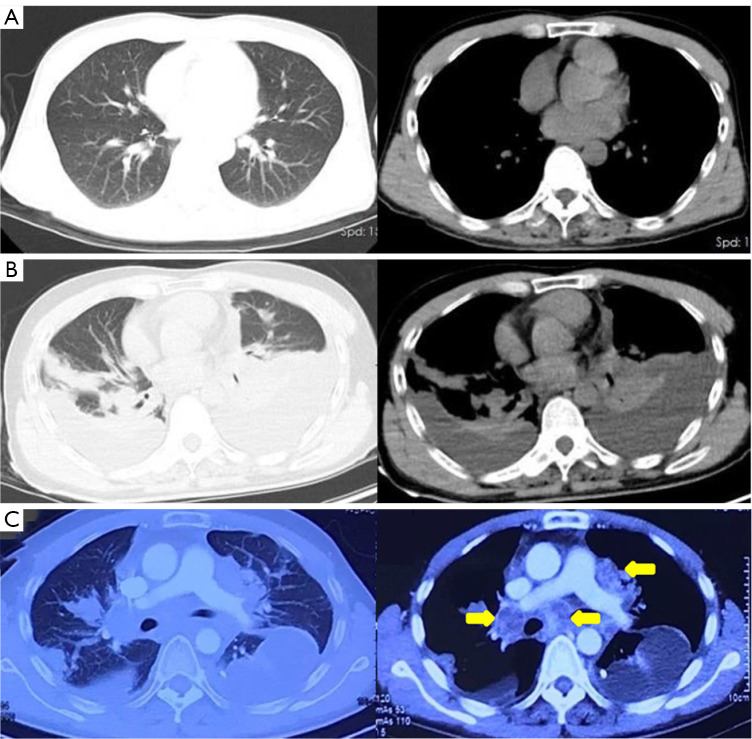
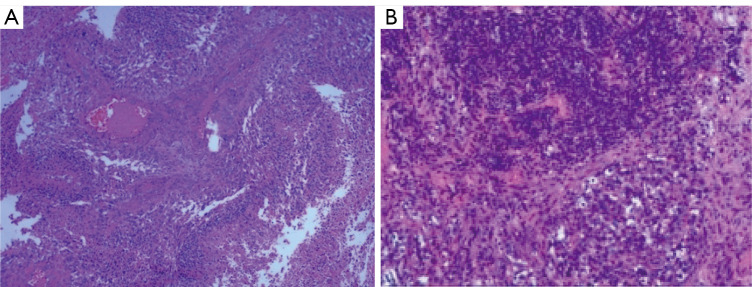
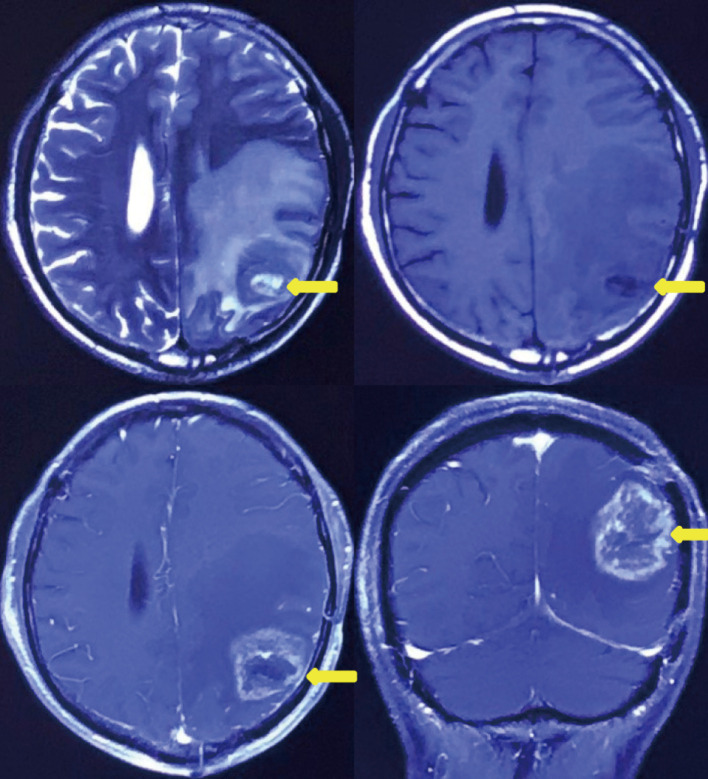
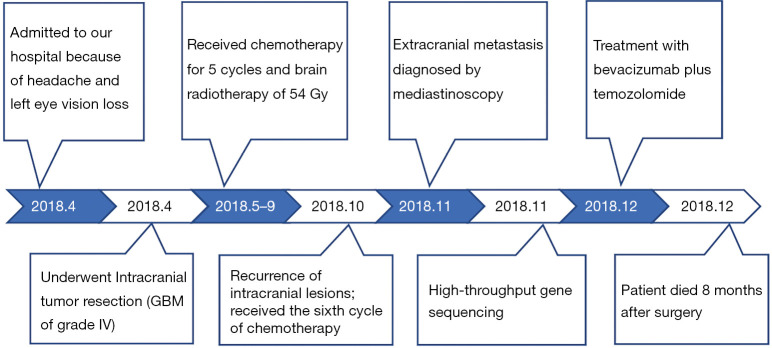
Case description: Here, we present a case of a male patient with headache and left eye vision loss for 2 months who had a left occipital lobe tumor. GBM of grade IV [isocitrate dehydrogenase 1 (IDH-1) wild type] was diagnosed based on the histological profiles of intracranial tumor according to the World Health Organization standard. ECM of GBM located in the mediastinal lymph node occurred 6 months after resection of the intracranial tumor. High throughput gene sequencing was performed using ECM lesions. Mutated genes included tumor protein 53 (TP53), CUB and Sushi multiple domains 3 (CSMD3), poly(ADP-ribose) polymerase family member 4 (PARP4), and PTEN. The patient underwent surgery, radiotherapy, chemotherapy, and anti-angiogenic drug treatment. Unfortunately, the patient died 8 months after surgery.
Conclusions: ECM of GBM is rare, and its prognosis is very poor. Mutated genes in ECM included TP53, CSMD3, PARP4, and PTEN in our case. Genomic analysis provides important insights into GBM and its ECM.
Keywords: Glioblastoma (GBM); case report; extracranial metastases (ECM); gene sequencing.
2022 Translational Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://tcr.amegroups.com/article/view/10.21037/tcr-22-955/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Pietschmann S, von Bueren AO, Kerber MJ, et al. An individual patient data meta-analysis on characteristics, treatments and outcomes of glioblastoma/ gliosarcoma patients with metastases outside of the central nervous system. PLoS One 2015;10:e0121592. 10.1371/journal.pone.0121592 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous