

Usefulness of the estimation of physiologic ability and surgical stress (E-PASS) system for prediction of complication and prognosis in hepatocellular carcinoma patients after hepatectomy
- PMID: 36093556
- PMCID: PMC9459632
- DOI: 10.21037/tcr-22-352
Usefulness of the estimation of physiologic ability and surgical stress (E-PASS) system for prediction of complication and prognosis in hepatocellular carcinoma patients after hepatectomy
Abstract
Background: Estimation of physiologic ability and surgical stress (E-PASS) system was verified in predicting postoperative complications or mortality in many surgical operations. This research aimed to investigate whether the E-PASS system could predict postoperative complications and was related with long-term prognosis in primary hepatocellular carcinoma (HCC) patients.
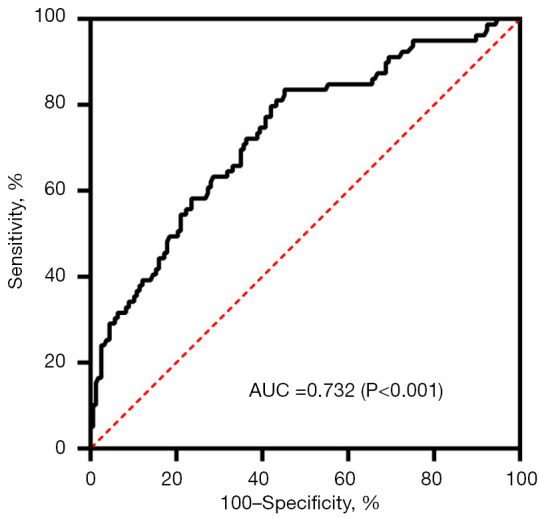
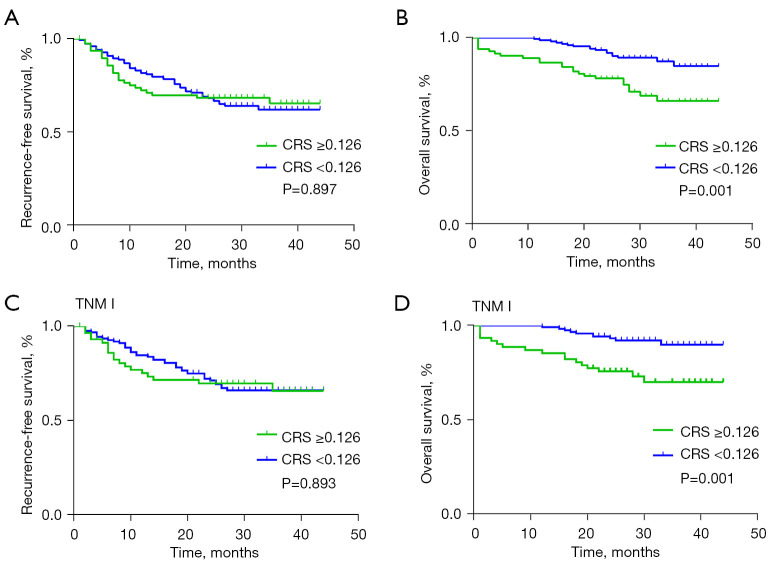
Methods: A total of 236 HCC patients who underwent liver resection were collected in this study. We performed univariate analyses to determine the potential risk factors for complications after hepatectomy. The potential independent risk factors were then included in the logistic regression for multivariable analysis. The optimal cutoff value of Comprehensive Risk Score (CRS) was identified by a receiver operating characteristic (ROC) curve. Based on this value, the patients were divided into two groups to investigate the relation between CRS with postoperative complications. The relation between CRS and overall survival (OS) or recurrence-free survival (RFS) was analyzed further in these two groups.
Results: Postoperative complications occurred in 79 patients. Multivariable analysis suggested that CRS was independent factor for predicting postoperative complications (P<0.001). The optimal CRS cutoff value in our study was 0.126. Patients with high Preoperative Risk Score (PRS) had a higher rate of postoperative complications occurrence, both major and mild complications (P<0.001). Our study showed that HCC patients with higher CRS had poorer survival prognosis [hazard ratio (HR): 3.735, 95% confidence interval (CI): 1.200-11.631, P=0.023]. The 3-year OS rate of high CRS group (CRS ≥0.126) and low CRS group (CRS <0.126) were 66.2% vs. 84.8% (P<0.001), respectively.
Conclusions: For HCC patients after liver resection, E-PASS was an effective predictive system for evaluating the risks of postoperative complications and may can predict prognosis in long term.
Keywords: Estimation of physiologic ability and surgical stress (E-PASS); hepatocellular carcinoma (HCC); postoperative complication; prognosis.
2022 Translational Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tcr.amegroups.com/article/view/10.21037/tcr-22-352/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Estimation of Physiologic Ability and Surgical Stress scoring system for predicting complications following abdominal surgery: A meta-analysis spanning 2004 to 2022.World J Gastrointest Surg. 2024 Jan 27;16(1):215-227. doi: 10.4240/wjgs.v16.i1.215. World J Gastrointest Surg. 2024. PMID: 38328319 Free PMC article.
-
The Estimation of Physiologic Ability and Surgical Stress (E-PASS) model as a predictor of postoperative complications and mortality after digestive surgeries: a meta-analysis and systematic review.Ann Palliat Med. 2021 Aug;10(8):8672-8683. doi: 10.21037/apm-21-941. Epub 2021 Aug 12. Ann Palliat Med. 2021. PMID: 34412493
-
E-PASS score as a useful predictor of postoperative complications and mortality after colorectal surgery in elderly patients.Int J Colorectal Dis. 2016 Feb;31(2):217-25. doi: 10.1007/s00384-015-2456-7. Epub 2015 Nov 26. Int J Colorectal Dis. 2016. PMID: 26607908
-
Is an estimation of physiologic ability and surgical stress able to predict operative morbidity after pancreaticoduodenectomy?J Hepatobiliary Pancreat Sci. 2010 Mar;17(2):132-8. doi: 10.1007/s00534-009-0116-4. Epub 2009 May 9. J Hepatobiliary Pancreat Sci. 2010. PMID: 19430714
-
[A new prognostic score system of hepatocellular carcinoma following hepatectomy].Zhonghua Zhong Liu Za Zhi. 2017 Dec 23;39(12):903-909. doi: 10.3760/cma.j.issn.0253-3766.2017.12.005. Zhonghua Zhong Liu Za Zhi. 2017. PMID: 29262506 Chinese.
Cited by
-
Evaluation of the up-to-7 criterion for determining the treatment of hepatocellular carcinoma in Barcelona Clinic Liver Cancer stage B: a single-center retrospective cohort study.J Gastrointest Oncol. 2023 Apr 29;14(2):768-779. doi: 10.21037/jgo-23-69. Epub 2023 Apr 11. J Gastrointest Oncol. 2023. PMID: 37201043 Free PMC article.
-
Estimation of Physiologic Ability and Surgical Stress scoring system for predicting complications following abdominal surgery: A meta-analysis spanning 2004 to 2022.World J Gastrointest Surg. 2024 Jan 27;16(1):215-227. doi: 10.4240/wjgs.v16.i1.215. World J Gastrointest Surg. 2024. PMID: 38328319 Free PMC article.
References
LinkOut - more resources
Full Text Sources