

The Lung Allocation Score Remains Inequitable for Patients with Pulmonary Arterial Hypertension, Even after the 2015 Revision
- PMID: 36094471
- PMCID: PMC9896647
- DOI: 10.1164/rccm.202201-0217OC
The Lung Allocation Score Remains Inequitable for Patients with Pulmonary Arterial Hypertension, Even after the 2015 Revision
Abstract
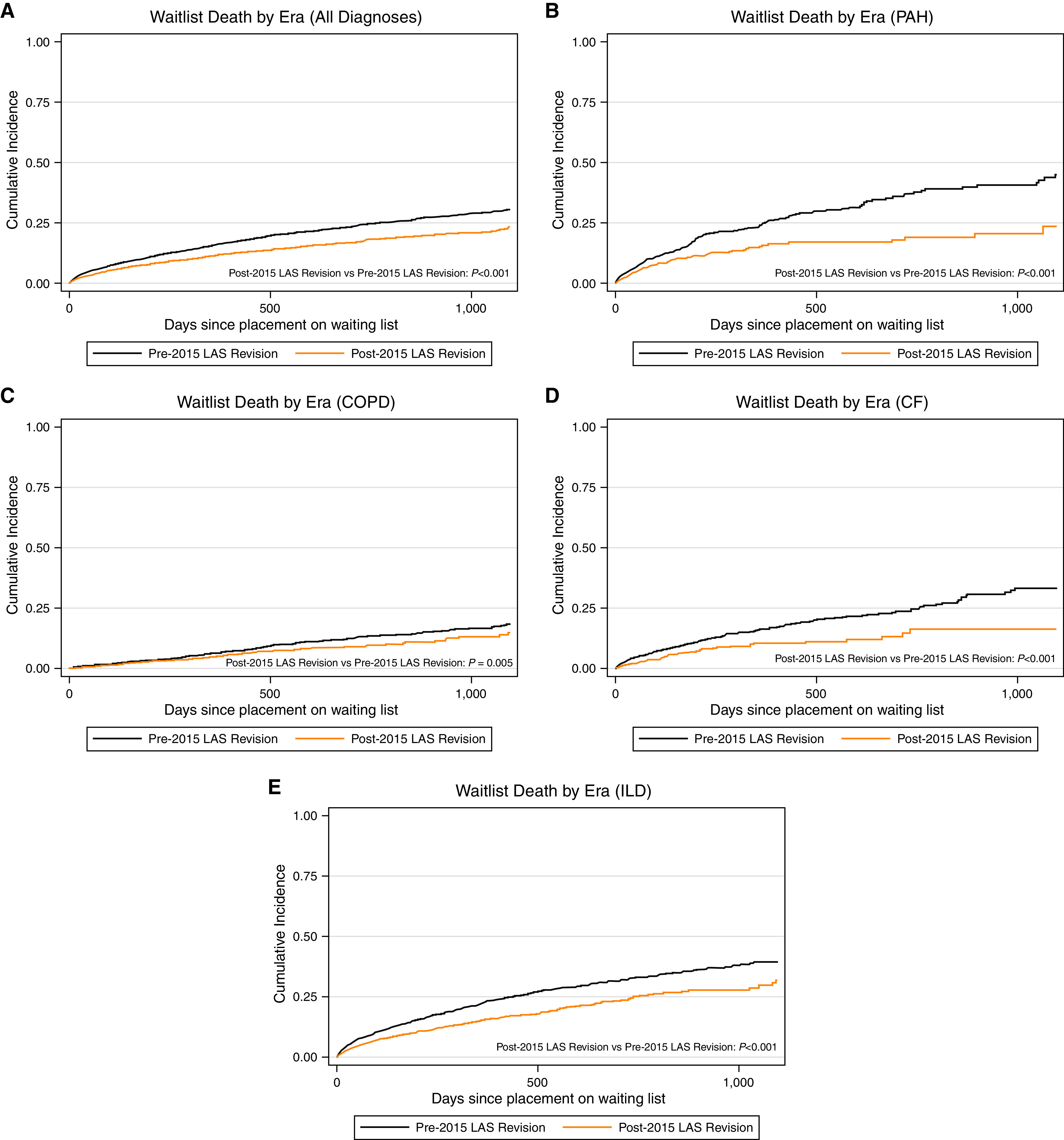
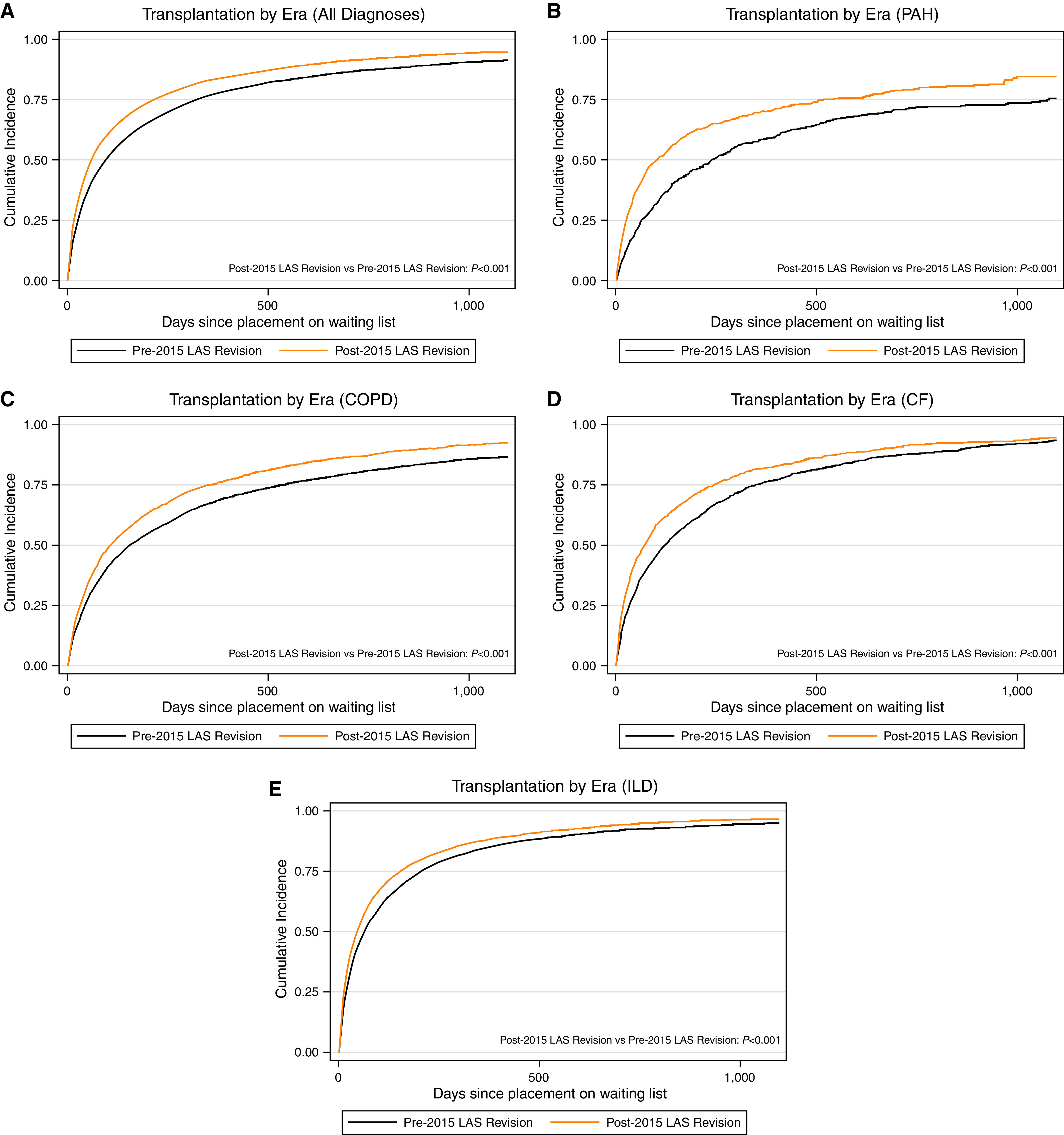
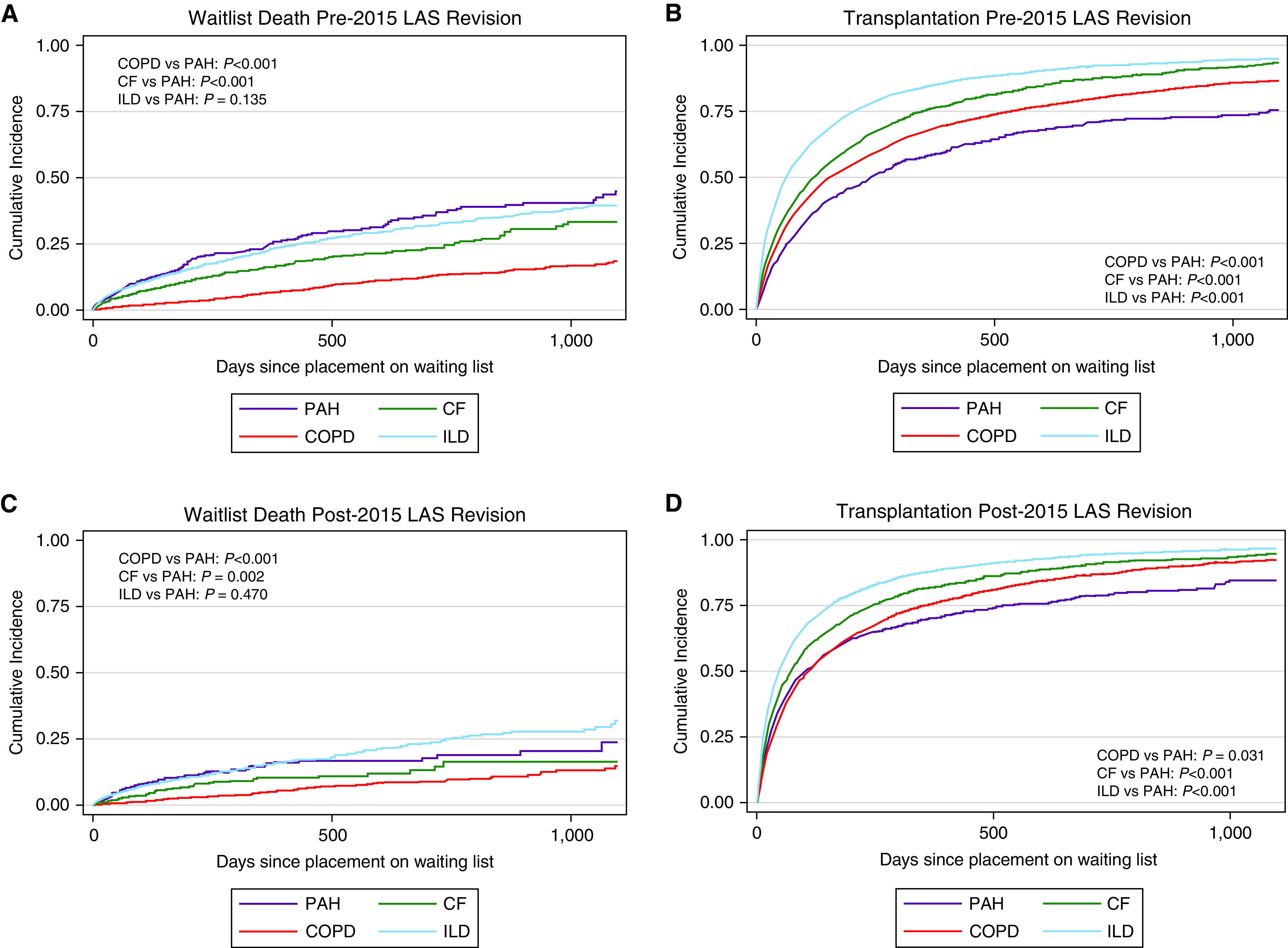
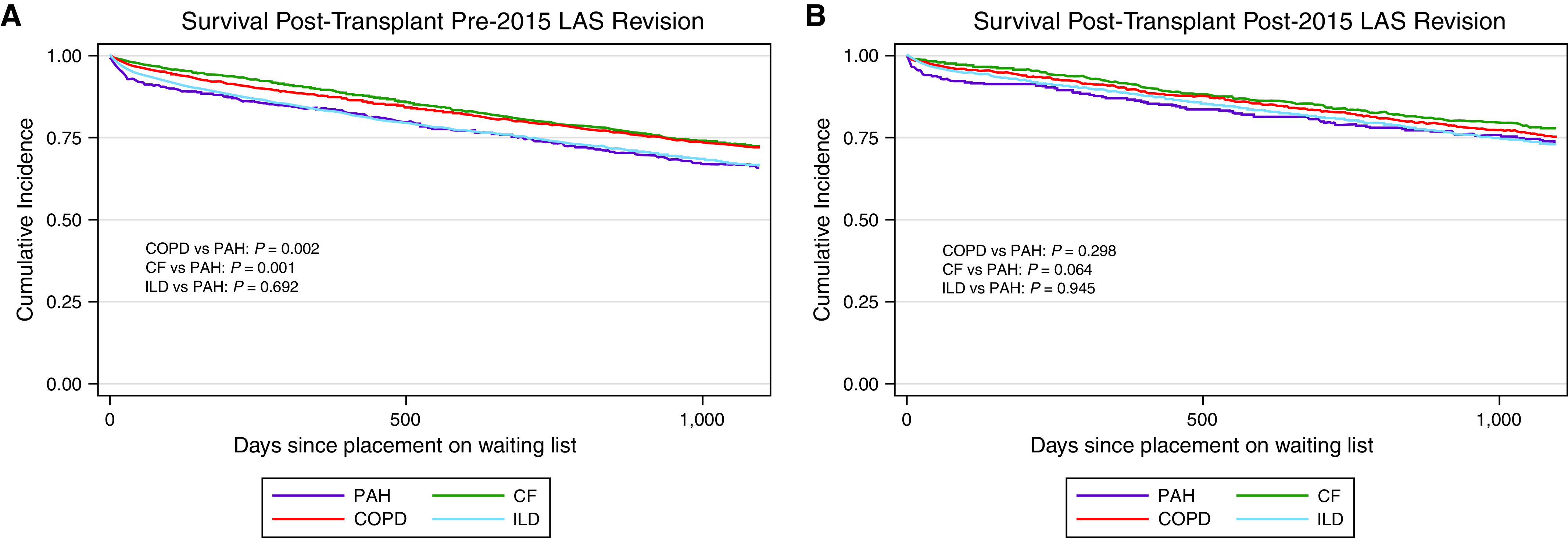
Rationale: The lung allocation score (LAS) was revised in 2015 to improve waiting list mortality and rate of transplant for patients with pulmonary arterial hypertension (PAH). Objectives: We sought to determine if the 2015 revision achieved its intended goals. Methods: Using the Standard Transplant Analysis and Research file, we assessed the impact of the 2015 LAS revision by comparing the pre- and postrevision eras. Registrants were divided into the LAS diagnostic categories: group A-chronic obstructive pulmonary disease; group B-pulmonary arterial hypertension; group C-cystic fibrosis; and group D-interstitial lung disease. Competing risk regressions were used to assess the two mutually exclusive competing risks of waiting list death and transplant. Cumulative incidence plots were created to visually inspect risks. Measurements and Main Results: The LAS at organ matching increased by 14.2 points for registrants with PAH after the 2015 LAS revision, the greatest increase among diagnostic categories (other LAS categories: Δ, -0.9 to +2.8 points). Before the revision, registrants with PAH had the highest risk of death and lowest likelihood of transplant. After the 2015 revision, registrants with PAH still had the highest risk of death, now similar to those with interstitial lung disease, and the lowest rate of transplant, now similar to those with chronic obstructive pulmonary disease. Conclusions: Although the 2015 LAS revision improved access to transplant and reduced the risk of waitlist death for patients with PAH, it did not go far enough. Significant differences in waitlist mortality and likelihood of transplant persist.
Keywords: equity; lung allocation score; lung transplantation; pulmonary arterial hypertension.
Figures
Comment in
-
Comparing the Incomparable: Identifying Common Themes Across a Diverse Landscape to Address Equity in Lung Allocation.Am J Respir Crit Care Med. 2023 Feb 1;207(3):236-238. doi: 10.1164/rccm.202209-1816ED. Am J Respir Crit Care Med. 2023. PMID: 36219486 Free PMC article. No abstract available.
References
-
- McGoon MD, Benza RL, Escribano-Subias P, Jiang X, Miller DP, Peacock AJ, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol . 2013;62:D51–D59. - PubMed
-
- Lau EMT, Giannoulatou E, Celermajer DS, Humbert M. Epidemiology and treatment of pulmonary arterial hypertension. Nat Rev Cardiol . 2017;14:603–614. - PubMed
-
- Foderaro A, Ventetuolo CE. Pulmonary arterial hypertension and the sex hormone paradox. Curr Hypertens Rep . 2016;18:84. - PubMed
-
- Shafazand S, Goldstein MK, Doyle RL, Hlatky MA, Gould MK. Health-related quality of life in patients with pulmonary arterial hypertension. Chest . 2004;126:1452–1459. - PubMed
