

COVID-19 Vaccine Booster Strategies in Light of Emerging Viral Variants: Frequency, Timing, and Target Groups
- PMID: 36094720
- PMCID: PMC9464609
- DOI: 10.1007/s40121-022-00683-z
COVID-19 Vaccine Booster Strategies in Light of Emerging Viral Variants: Frequency, Timing, and Target Groups
Abstract
Background: Vaccinations have reduced severe burden of COVID-19 and allowed for lifting of non-pharmaceutical interventions. However, with immunity waning alongside emergence of more transmissible variants of concern, vaccination strategies must be examined.
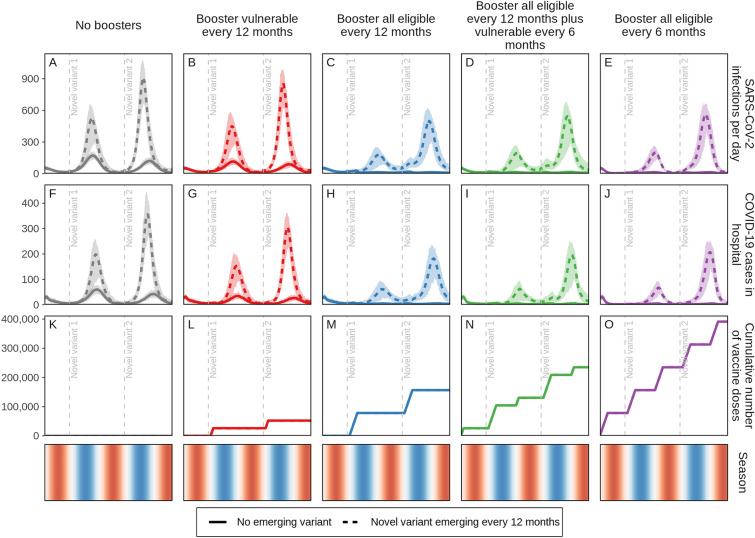
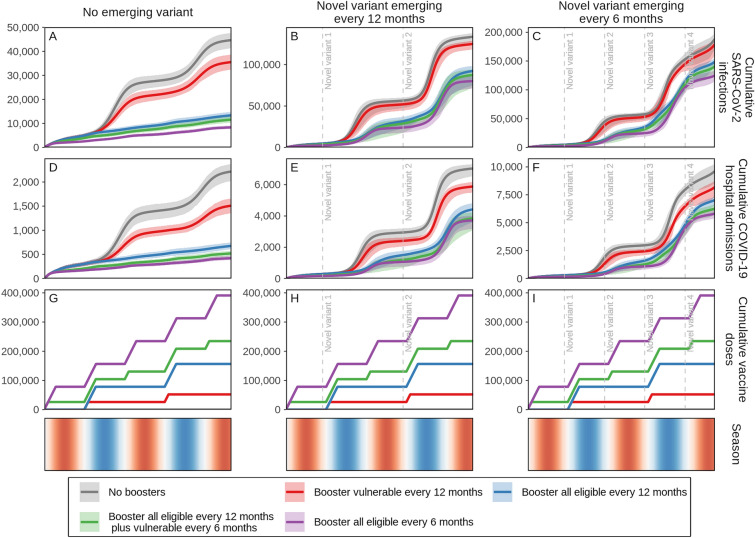
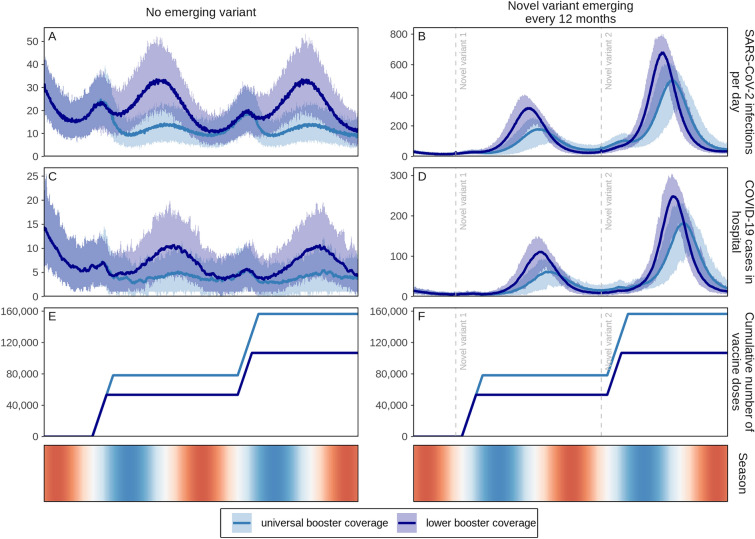
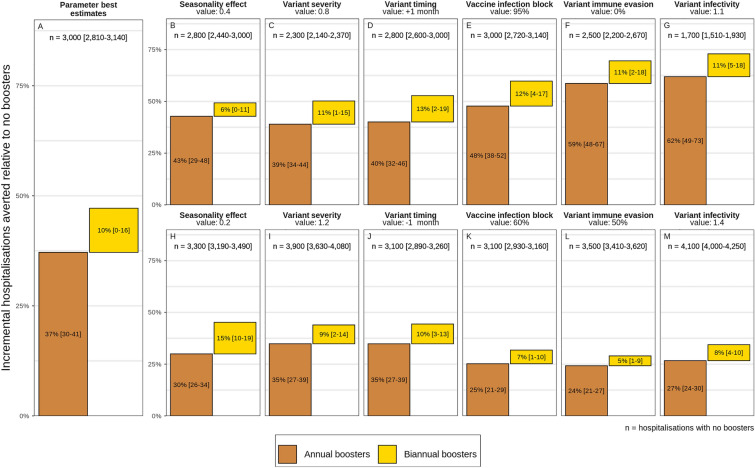
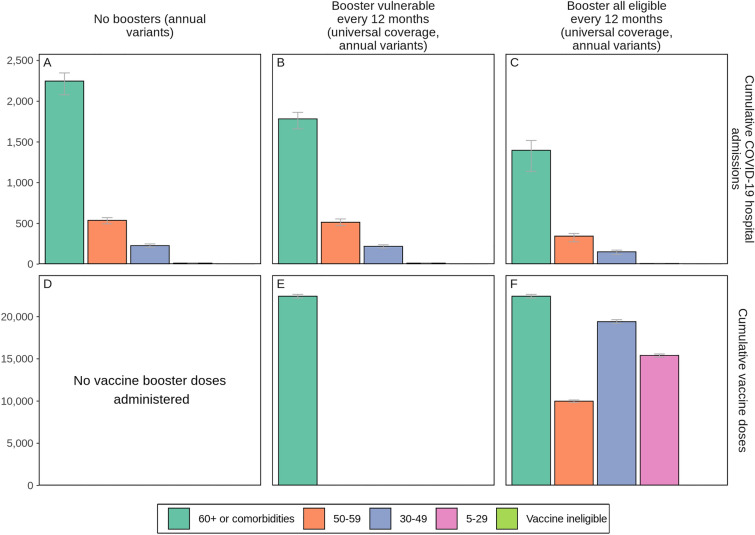
Methods: Here we apply a SARS-CoV-2 transmission model to identify preferred frequency, timing, and target groups for vaccine boosters to reduce public health burden and health systems risk. We estimated new infections and hospital admissions averted over 2 years through annual or biannual boosting of those eligible (those who received doses one and two) who are (1) most vulnerable (60+ or living with comorbidities) or (2) those 5+, at universal (98% of eligible) or lower coverage (85% of those 50+ or with comorbidities and 50% of 5-49 year olds) representing moderate vaccine fatigue and/or hesitancy. We simulated three emerging variant scenarios: (1) no new variants; (2) 25% more infectious and immune-evading Omicron-level severity variants emerge annually and become dominant; (3) emerge biannually. We further explored the impact of varying seasonality, variant immune-evading capacity, infectivity, severity, timing, and vaccine infection blocking assumptions.
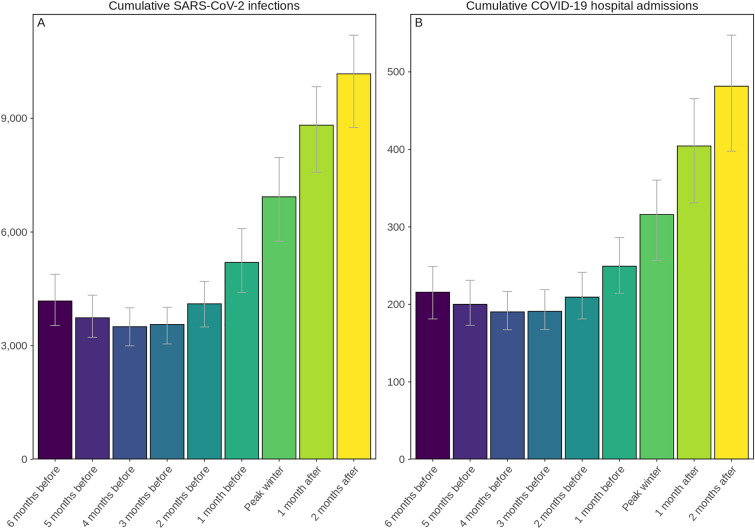
Results: To reduce COVID-19-related hospitalisations over the next 2 years, boosters should be provided for all those eligible annually 3-4 months ahead of peak winter whether or not new variants of concern emerge. Only boosting those most vulnerable is unlikely to ensure reduced stress on health systems. Moreover, boosting all eligible better protects those most vulnerable than only boosting the vulnerable group. Conversely, while this strategy may not ensure reduced stress on health systems, as an indication of cost-effectiveness, per booster dose more hospitalisations could be averted through annual boosting of those most vulnerable versus all eligible, since those most vulnerable are more likely to seek hospital care once infected, whereas increasing to biannual boosting showed diminishing returns. Results were robust when key model parameters were varied. However, we found that the more frequently variants emerge, the less the effect boosters will have, regardless of whether administered annually or biannually.
Conclusions: Delivering well-timed annual COVID-19 vaccine boosters to all those eligible, prioritising those most vulnerable, can reduce infections and hospital admissions. Findings provide model-based evidence for decision-makers to plan for administering COVID-19 boosters ahead of winter 2022-2023 to help mitigate the health burden and health system stress.
Keywords: Booster; COVID-19; Immunity; Modelling; SARS-CoV-2; Vaccination.
© 2022. The Author(s).
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard Geneva: WHO; 2022. https://covid19.who.int/. Accessed 28 May 2022.
-
- Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022;399(10332):1303–1312. doi: 10.1016/S0140-6736(22)00462-7. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
